Download
1 / 1
10 likes | 73 Views
However, many participants identified specific difficulties. “I’m afraid that I feel that I can’t do much about fostering a good relationship between the doctor and me because I think that’s something they don’t teach in university and [doctors] don’t learn it in medical school.”.

E N D
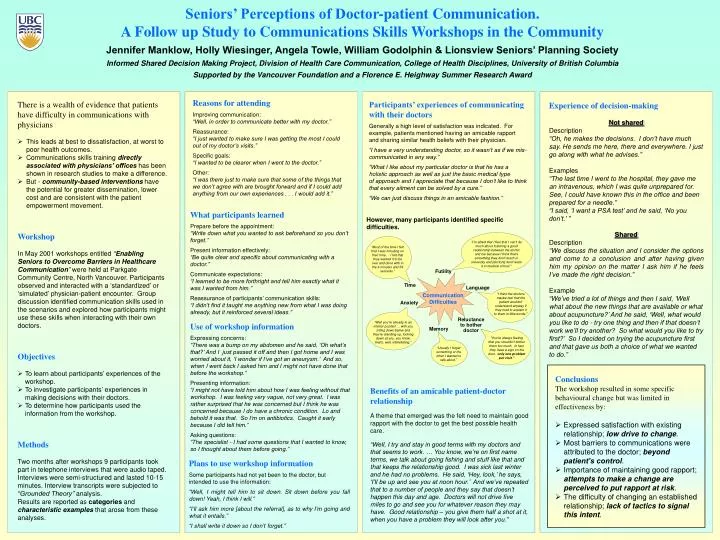
However, many participants identified specific difficulties. “I’m afraid that I feel that I can’t do much about fostering a good relationship between the doctor and me because I think that’s something they don’t teach in university and [doctors] don’t learn it in medical school.” “Most of the time I felt that I was intruding on their time ... I felt that they wanted it to be over and done with in the 4 minutes and 59 seconds.” Futility Time Language “I think the doctors maybe feel that the patient wouldn’t understand anyway if they tried to explain it to them in little words.” Communication Difficulties Anxiety Reluctance to bother doctor “Well you’re already in an inferior position ... with you sitting down below and they’re standing up, looking down at you, you know, that’s, well, intimidating.” Memory “You’re always feeling that you shouldn’t bother them too much. In fact, they have a sign on the door, ‘only one problem per visit.’” “Usually I forget something or the other I wanted to talk about.” Seniors’ Perceptions of Doctor-patient Communication.A Follow up Study to Communications Skills Workshops in the Community Jennifer Manklow, Holly Wiesinger, Angela Towle, William Godolphin & Lionsview Seniors’ Planning Society Informed Shared Decision Making Project, Division of Health Care Communication, College of Health Disciplines, University of British Columbia Supported by the Vancouver Foundation and a Florence E. Heighway Summer Research Award Reasons for attending Improving communication: “Well, in order to communicate better with my doctor.” Reassurance: “I just wanted to make sure I was getting the most I could out of my doctor’s visits.” Specific goals: “I wanted to be clearer when I went to the doctor.” Other: “I was there just to make sure that some of the things that we don’t agree with are brought forward and if I could add anything from our own experiences . . . I would add it.” • There is a wealth of evidence that patients • have difficulty in communications with • physicians • This leads at best to dissatisfaction, at worst to poor health outcomes. • Communications skills training directly associated with physicians’ offices has been shown in research studies to make a difference. • But - community-based interventions have the potential for greater dissemination, lower cost and are consistent with the patient empowerment movement. Participants’ experiences of communicating with their doctors Generally a high level of satisfaction was indicated. For example, patients mentioned having an amicable rapport and sharing similar health beliefs with their physician. “I have a very understanding doctor, so it wasn’t as if we mis-communicated in any way.” “What I like about my particular doctor is that he has a holistic approach as well as just the basic medical type of approach and I appreciate that because I don’t like to think that every ailment can be solved by a cure.” “We can just discuss things in an amicable fashion.” Experience of decision-making Not shared Description “Oh, he makes the decisions. I don’t have much say. He sends me here, there and everywhere. I just go along with what he advises.” Examples “The last time I went to the hospital, they gave me an intravenous, which I was quite unprepared for. See, I could have known this in the office and been prepared for a needle.” “I said, ‘I want a PSA test’ and he said, ‘No you don’t.’ ” Shared Description “We discuss the situation and I consider the options and come to a conclusion and after having given him my opinion on the matter I ask him if he feels I’ve made the right decision.” Example “We’ve tried a lot of things and then I said, ‘Well what about the new things that are available or what about acupuncture?’ And he said, ‘Well, what would you like to do - try one thing and then if that doesn’t work we’ll try another? So what would you like to try first?’ So I decided on trying the acupuncture first and that gave us both a choice of what we wanted to do.” What participants learned Prepare before the appointment: “Write down what you wanted to ask beforehand so you don’t forget.” Present information effectively: “Be quite clear and specific about communicating with a doctor.” Communicate expectations: “I learned to be more forthright and tell him exactly what it was I wanted from him.” Reassurance of participants’ communication skills: “I didn’t find it taught me anything new from what I was doing already, but it reinforced several ideas.” Workshop In May 2001 workshops entitled “Enabling Seniors to Overcome Barriers in Healthcare Communication” were held at Parkgate Community Centre, North Vancouver. Participants observed and interacted with a ‘standardized’ or ‘simulated’ physician-patient encounter. Group discussion identified communication skills used in the scenarios and explored how participants might use these skills when interacting with their own doctors. Use of workshop information Expressing concerns: “There was a bump on my abdomen and he said, ‘Oh what’s that?’ And I just passed it off and then I got home and I was worried about it, ‘I wonder if I’ve got an aneurysm.’ And so, when I went back I asked him and I might not have done that before the workshop.” Presenting information: “I might not have told him about how I was feeling without that workshop. I was feeling very vague, not very great. I was rather surprised that he was concerned but I think he was concerned because I do have a chronic condition. Lo and behold it was that. So I’m on antibiotics. Caught it early because I did tell him.” Asking questions: “The specialist - I had some questions that I wanted to know, so I thought about them before going.” • Objectives • To learn about participants’ experiences of the workshop. • To investigate participants’ experiences in making decisions with their doctors. • To determine how participants used the information from the workshop. • Conclusions • The workshop resulted in some specific • behavioural change but was limited in • effectiveness by: • Expressed satisfaction with existing relationship; low drive to change. • Most barriers to communications were attributed to the doctor; beyond patient’s control. • Importance of maintaining good rapport; attempts to make a change are perceived to put rapport at risk. • The difficulty of changing an established relationship; lack of tactics to signal this intent. Benefits of an amicable patient-doctor relationship A theme that emerged was the felt need to maintain good rapport with the doctor to get the best possible health care. “Well, I try and stay in good terms with my doctors and that seems to work. … You know, we’re on first name terms, we talk about going fishing and stuff like that and that keeps the relationship good. I was sick last winter and he had no problems. He said, ‘Hey, look,’ he says, ‘I’ll be up and see you at noon hour.’ And we’ve repeated that to a number of people and they say that doesn’t happen this day and age. Doctors will not drive five miles to go and see you for whatever reason they may have. Good relationship – you give them half a shot at it, when you have a problem they will look after you.” Methods Two months after workshops 9 participants took part in telephone interviews that were audio taped. Interviews were semi-structured and lasted 10-15 minutes. Interview transcripts were subjected to “Grounded Theory” analysis. Results are reported as categories and characteristic examples that arose from these analyses. Plans to use workshop information Some participants had not yet been to the doctor, but intended to use the information: “Well, I might tell him to sit down. Sit down before you fall down! Yeah, I think I will.” “I’ll ask him more [about the referral], as to why I’m going and what it entails.” “I shall write it down so I don’t forget.”