Download
1 / 59
770 likes | 1.76k Views
Pleural Disease. G Saydain MD, Assistant Prof. Of Medicine Pulmonary Critical Care and Sleep Division Wayne State University. Pleural disease: Learning Objectives. Physiology of pleural space Accumulation of pleural fluid Identify differences between a transudate and exudate

E N D
Pleural Disease G Saydain MD, Assistant Prof. Of Medicine Pulmonary Critical Care and Sleep Division Wayne State University
Pleural disease: Learning Objectives • Physiology of pleural space • Accumulation of pleural fluid • Identify differences between a transudate and exudate • Causes of transudates/exudates • Diagnostic work up for pleural effusion • Management of common causes of pleural effusion • Pneumothorax • Pleural tumors
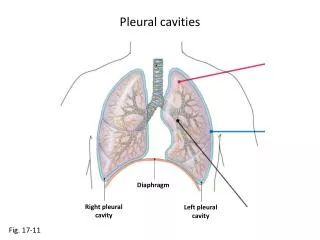
Pleura : Physiology • Allows extensive movement of Lungs relative to chest wall • Mechanical support for the lungs • Limits lung expansion • Contributes to the work of deflation • Distributes the negative forces of inflation evenly
Pleural Fluid • Normally 1-3 cc • Role: lung-chest wall interaction • Pathologic Increase = Effusion • Increased hydrostatic forces • Decreased oncotic forces • Disease of the pleura, capillaries and/or underlying lung
Pathology • Effusions - collection of fluid • Pneumothorax – collection of water • Fibrothorax – scar pleura cannot expand • Tumors - rare
Pleural Fluid : Transudate • Leakage of Fluid from pleura or decreased reabsorption • Increased Hydrostatic pressure • Decrease in Oncotic pressure • Leakage from peritoneum
Pleural Effusion : Exudates • Pleural injury due to inflammation, infection, or malignancy when a high-protein lung edema leaks into the pleural space. Pneumonia or pulmonary embolism, Cancer or SLE • Leakage from surrounding tissues Mediastinum (esophageal rupture or chylothorax), Retroperitoneum (pancreatic pseudocyst), Peritoneum (ascites with spontaneous bacterial peritonitis )
Common Causes of Pleural effusion in USA • Congestive heart failure 500,000 • Pneumonia (bacterial) 300,000 • Malignant disease 200,000 • Pulmonary embolization 150,000 • Viral disease 100,000 • Post-coronary artery bypass surgery 60,000 • Cirrhosis with ascites 50,000
Symptoms & Signs of Pleural effusion • Cough • Chest pain • Dyspnea • Decreased chest wall movement • Dullness to percussion • Diminished or absent breath sounds • Tracheal/mediastinal shift to other side in large effusions
Diagnosis of Pleural effusion CXR PA view Lateral Decubitus CT Scan Ultra Sound
48 year old Hispanic American male developed cough , fever, chills and right chest pain 2 weeks after returning from a 4 week vacation in Chili
Diagnostic Evaluation of Pleural EffusionAscertain Etiology • Diagnosis can be made in Up to 75% of pleural effusions 25% diagnostic 50% Presumptive diagnosis • In significant number of case exclusion of certain diagnoses may be possible
Thoracentesis Diagnostic Therapeutic -Contraindications lack of patient cooperation Uncorrected Severe coagulopathy; Hemodynamic or rhythm instability Unstable angina. Local chest wall infection
Thoracentesis : Procedure • Patient sitting comfortably, leaning slightly forward, and resting the arms on a support. • The needle must be inserted in an intercostal space overlying the fluid • The space is usually one interspace below the fluid level, in the midscapular line • May use ultrasound for localization
Thoracentesis :Complications • Pneumothorax • Hemorrhage • Vasovagal or simple syncope; • Infection • puncture of the spleen or liver due to low or unusually deep needle insertion; and • Reexpansion pulmonary edema, with rapid removal of > 1 L of pleural fluid.
Diagnostic Evaluation of Pleural Fluid • Inspection/observation • Cell Count and differential • Protein • Glucose • pH • LDH • Gram Stain & Culture • AFB stain & Culture (TB) • Cytology for malignant cells
Pleural Fluid diagnostic evaluation : Other tests • Amylase - pancreatitis • Triglyceride • Cholesterol • Bilirubin – liver failure • Creatinine – kidney failure
Observation of pleural fluid color • Pale Transudate • Pus Empyema • Red Malignancy, post cardiac surgery inj. Synd • Pulmonary infarction • Trauma Hemothorax
Observation of Pleural Fluid Characteristic features • Viscous Mesotheleoma (Aesbestos?) • Turbid Inflammatory/lipid (Pus?) • Brown Long standing bloody eff. • Black Aspergillosis
Transudate Vs Exudate • L D H >2/3 rd the upper limits of normal for • Lab sr.. LDH value = Exudate
Pleural Fluid Analyisis Transudate Exudate Cell Type Infections Neoplsatic Drugs/Doctors Immunologic All others CHF Nephrotic Syndrome Cirrhosis Low Glucose High LDH Microbiology Cytology Special Tests
Some Typical associations • Pleural fl. LDH >1000 iu/L : empyema, rheumatoid, malignancy • Low Glucose : Empyema, malignancy, Rheumatoid arthritis , TB • pH: < 7.1 = complicated parapneumonic/malignancy /Esophegial Rupture • Amylase (esophagus, pancreas) • Lipids • Tryglycerides: milky, chylous • Cholesterol: nonspecific
Cell Count in Pleural Fluid • WBC: > 50,000/ ŭ L (mostly polymorphs)complicated parapneumonic effusion > 10,000 cells/ ŭ L Bacterial pneumonia, ac. pancreatitis, lupus < 5000 cells/ ŭ L Tuberculosis & Malignancy Lymphocytosis TB, Malignancy Rheumatoid pleurisy, SLE
Transdute Pleural Effusions • Congestive Heart Failure. Commonest cause. • Cirrhosis Usually with ascitis • Neph. Syndrome Low Albumin • Hypoprotenemia Low Albumin • Peritoneal Dialysis ( if Exudate suspect peritonitis) Treatment • Treat the underlying cause • Therapeutic Drainage : for large effusion with sever dyspnea
Exudates • Infections : Pneumonia, TB • Malignancies Mostly metastastic Lung, Breast • Connective Tissue Disease • Other: pancreatitis, post-cardiac injury syndrome, trauma, P.E., pneumothorax, subphrenic abscess, etc.
Effusions associated with Pneumonia • 36-57% of pneumonia associated with pleural effusion • Usually Simple parapneumonic effusions • Resolve spontaneously • Complicated effusions may proceed to develop simple or multiple loculations or Empyema (pus in pleural cavity) • Thoracentesis to be done almost always for effusions with pneumonia.
Para Pneumonic Pleural Effusion PPE Phases R E S O L U T I O N E M P Y E M A Exudative Fibrinopurulant Complete resolution Organization
Parapneumonic Pleural Effusion High Risk • Require second procedure • Poor outcome Prolonged hospitalization Systemic toxicity Increased morbidity with second procedure Increased risk for ventilatory impairment Risk of local spread of infection • Single most important factor determining outcome : delay in seeking medical intervention
Features of Complex/Complicated Parapneumonic effusion • Low pH, Low glucose, • High LDH , High WBC count (thousands) • Positive gram stain/culture • Frank pus …..empyema • Loculated
Treatment for Complex/complicated effusion • In addition to antibiotics patient may need a drainage procedure. • No major loculations: Chest tube placement • Many loculations : Fibrinolytic therapy (not effective usually) Thoracoscopy or Surgical Decortication
Suspected Malignancy • Cytology • Pleural biopsy may be required • T/B lymphocytes
Rheumatologic Diseases • Appearance, low glucose • Immunologic studies • RF > 1:320 • LE cells • ANA > 1:160 • Low complement: active
No Diagnosis • Up to 20%: no specific dx • Most: eventually TB or malignancy • Practical management: • Empiric anti TB treatment • Keep evaluation reasonable • Careful follow-up clinically
Role of Pleural Biopsy • Tuberculosis • Caseating granulomas, AFB + • Bx + fluid + cultures: 75-80% • Malignancy • Scattered distribution (lower yield) • Rarely: other diseases
Pneumothorax • Air in the pleural space • Penetration of the chest wall • Trauma • Iatrogenic (by doctors) • Leak from lung tissue • Lung disease • Airway • barotrauma
Pneumothorax • Air in pleural Cavity • Pressure increases in tension pneumothorax • Can cause: • Hypotension • Collapse of lung • Decreased Pao2 due to shunt/alveolar hypoventilation
Clinical Features • Chest pain ; usually sudden onset • Dyspnea • Hypotension • Shift of trachea to other side • Resonant percussion note (tympanic) • Diminished or absent breath sounds • Suspect after a procedure (e.g sub-clavian or internal jugular line placement )
Spontaneous Pneumothorax • No known cause • Diagnosis : CXR • Small pleural effusion in 15% Recurrence • Greatest in the month immediately following • 23% over 5 years
Spontaneous Pneumothorax • Annual incidence of 8600 in USA • 7.4/100000 in men • 1.2/100000 in women Etiology • Emphysematous changes in apical fields • Smoking • Patients tend to be taller / thinner • Autosomal Dominant with 20% penetrance
Pneumothorax: Treatment • Observation < 15% PTX, 1.25% of hemithorax absorbed /day • Supplemental Oxygen\ • Simple Aspiration • Tube Thoracostomy • Sclerotherapy for reoccurant pneumothorax to create artificial fibrosis wiith talk • Open thoracotomy