Download
1 / 33
330 likes | 707 Views
Blood Cell Differentials. Laboratory Procedures. Let’s Review: Blood Composition. Separates into three components: Red Blood Cells (RBC’s) White Blood Cells and platelets (buffy coat) Plasma Bottom 1/3 to ½ of tube contains the heaviest of cellular material (the RBC’s). Blood films.

E N D
Blood Cell Differentials Laboratory Procedures
Let’s Review: Blood Composition Separates into three components: Red Blood Cells (RBC’s) White Blood Cells and platelets (buffy coat) Plasma Bottom 1/3 to ½ of tube contains the heaviest of cellular material (the RBC’s).
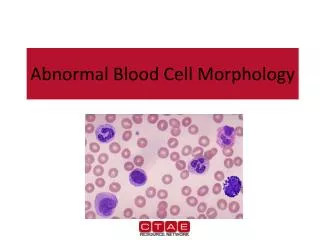
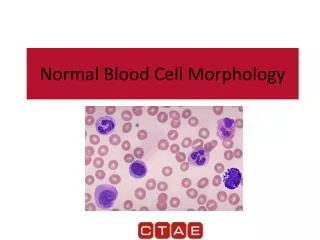
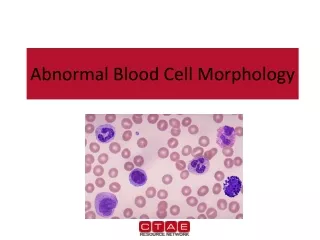
Blood films • The blood film is used to perform the differential WBC count; estimate platelet numbers; and evaluate the morphological features of WBCs, RBCs and platelets. • Wedge smears are prepared by placing a small drop of blood on a clean glass microscope slide
Staining a slide • Always stain using the lightest to darkest stain. • Remember which side of your slide is up (clothes pins are marked “top”) • Rinse off from back side of slide • May heat fix to speed up process.
Performing the Differential Cell Count • This is where the different white blood cells are tallied separately. This can be done by a blood counting machine, or by hand. • To manually count the different cells, first you must make a perfect slide. Stain the slide once it is dry. • Using a cell counter you will tally a total of 100 cells (this will make it easy to turn the numbers into a %)
Hematocrit - PCV • In the CBC, we determine the number of RBC’s in several different ways. The quickest and easiest is called the hematocrit, also referred to as the packed cell volume (PCV). • The hematocrit or the packed cell volume will tell you if the animal is dehydrated or anemic.
Whole blood is collected in an anticoagulant, such as EDTA or heparin and place in a capillary tube (75 mm). Microhematocrit tubes should be filled, with one ended plugged with clay sealant
A blood sample is placed in a tiny glass tube and spun in a centrifuge for 2-5 minutes. • Lie the tube in the centrifuge Hct head with plugged end to the outside, note the number of your slot. Ensure that a balancing hematocrit tube is placed opposite, either by someone placing their tube there, or by adding an empty tube • The cells are heavier than the plasma and are compacted at one end of the tube.
Special hematocrit tube have a linear scale, so the amount of blood in the tube need to be exact • The bottom of the RBC layer should be at the zero line and the top of the plasma on the top line (page 37 Fig 2-7) • PCV is determined as the percentage of the cellular portion relative to the total amount of blood in the tube
Plasma • Plasma color and transparency may be helpful in the determination of a diagnosis and should be recorded • Normal plasma is clear and a pale straw –yellow color • Page 36
Plasma Protein Concentration • Plasma Protein concentrations estimation by refractometry is is an important component of the CBC in all species • The plasma used to determinate the PCV is collected by breaking the hematocrit tube just above the Buffy coat- plasma interface
The plasma is allowed to flow onto the refractometer prism. • Page 37 fig 2-9
Anemia Literally means “no blood” but clinically means low total blood hemoglobin. Absolute anemia: most common, caused by failure to produce adequate numbers of cells or by a loss of cells at a rate greater than can be produced.
Clinical Signs of Anemia Pale mucous membranes Exercise intolerance Tachycardia Panting Icterus if anemia is caused by RBC breakdown in bloodstream.
Classification of Anemia • By RBC size (MCV): • Macrocytic • Erythrocytes are larger than normal. • Usually in the presence of regenerative anemia. • May be seen in FeLv • May see anisocytosis • Normocytic • Microcytic • Cells are smaller than normal which has been determined by Mean Cell Volume (MCV). • Usually occurs with iron deficiency caused by chronic blood loss or parasitism • By Hemoglobin concentration (MCHC) • Hypochromatic • RBC’s have decreased density of the characteristic hemoglobin color. • Frequently observed in iron deficiency caused by chronic blood loss or parasitism. • Normochromatic
Classification According to Bone Marrow Response • Regenerative anemia: • Characterized by evidence of increased production and delivery of new erythrocytes into circulation. • Usually suggests an extra bone marrow cause (blood loss, hemolysis, etc.)., • Diagnosis: • Peripheral blood smear. • Will see macrocytosis, polychromasia with Wright’s stain, reticulocytosis with methylene blue stain, may also see increased numbers of nucleated RBC’s
Nonregenerative anemia: • Indicates anemia is result of bone marrow defect. • No response evident in peripheral blood. • Marrow examination may be helpful with the diagnosis.
Types of Anemia Blood Loss Anemia Results from excessive hemorrhage although source can be subtle. Must determine if blood loss is internal or external. Possible causes: Trauma Persistent bleeding lesions Thrombocytopenia Coagulopathies Heavy parasitism Iatrogenic causes
Acute Blood Loss Anemia due to loss of blood in a sudden episode. All RBC parameters are normal for the first 12 hours. Hypovolemic shock can be apparent prior to a decreased PCV. Anemia will be normocytic, normochromatic, and apparently unresponsive with a low CRC. By day 4-5, the retic count increases and the anemia appears responsive.
Chronic Blood Loss Blood is lost slowly and continuously for a period of time. Body compensates for anemia by lowering oxygen-hemoglobin affinity, preferential shunting of blood to vital organs, increased cardiac output (tachycardia), and increased levels of erythropoietin. Anemia remains unresponsive unless iron stores are depleted. With decreasing iron stores, erythropoiesis is limited and RBC’s become smaller and deficient in Hgb (microcytic and hypochromic). Clinical signs include lethargy, weakness, decrease exercise tolerance, anorexia, pallor, lack of grooming, mild systolic murmur. Results in iron deficiency
Hemolytic Anemias Result of increased erythrocyte destruction within the body. Intravascular hemolysis: desctruction of erythrocyctes within the blood vessels and loss of Hgb from the cells. Extravascular hemolysis: RBC’s are lysed following phagocytosis.
Blood Borne Parasites Can produce anemia through hemolysis Parasites attach to erythrocyte membrane and cause increased destruction of the cells. May have symptoms of non-specific weight loss, anorexia, fever, etc. Babesia Ehrlichiosis
Toxin Induced Anemia/Heinz Body Hemoglobin denatures and forms Heinz bodies. Onion toxicity, Acetaminophen toxicity
Von Willebrand’s Disease Canine vWD is the most common inherited blood disorder. Von Willebrand’s Factor promotes platelet clumping in healthy dogs. Lack of this factor will cause a bleeding disorder. Dobies, German Sheperds, and Labs most common.