Download
1 / 27
270 likes | 488 Views
update in metastatic breast cancer. Dr.Mina Tajvidi Radiation oncologist. Fewer than 10 percent of women present with metastatic disease at the time of diagnosis

E N D
update in metastatic breast cancer Dr.MinaTajvidi Radiation oncologist
Fewer than 10 percent of women present with metastatic disease at the time of diagnosis the majority of women who relapse after definitive therapy for early stage or locally advanced disease will do so with disseminated metastatic disease rather than an isolated local recurrence The most common sites of distant tumor involvement are the bones, liver, and lungs.
Only 5 to 10 percent of patients with MBC survive five or more years, and perhaps 2 to 5 percent become long-term survivors, possibly cured of disease. In the absence of dramatic survival benefits, the focus of treatment in patients with MBC is Successful palliative therapy requires a reduction in disease-related symptoms without excessive treatment-related toxicity.
Selection of initial therapy Some patients are willing to accept a high burden of toxicity for small survival benefits, while others may only wish to be treated if toxicity is minimal and the likelihood of symptom control is high
Local versus systemic treatment Women who have an isolated local recurrence or involvement of a single metastatic site (eg, a single painful bone lesion or evidence of impending fracture) might be optimally palliated with local treatment alone, withholding systemic therapy until relapse or progression women with widespread disease involving multiple symptomatic sites are better served with initial systemic treatment. Systemic and local therapy are frequently combined. Bone targeting radioisotopes (eg, 89-strontium, 153-samarium lexodronam) are more often used in men with advanced prostate cancer, but they can provide excellent palliation of bone pain in women with predominantly osteoblastic multifocal bone metastases in whom pain control is not adequately controlled with radiation therapy, systemic antitumor therapy or analgesics.
Endocrine therapy versus chemotherapy for HER2-negative disease In general, the risk to benefit ratio is more favorable with endocrine therapy as compared to chemotherapy, due to a lower toxicity profile. If a patient with slowly progressive disease, no visceral involvement, and minimal symptoms, might be best served with a trial of endocrine therapy, even if her tumor has low or absent ER expression. a patient with rapidly-growing disease, especially with involvement of lung and/or liver, is better initially treated with chemotherapy, which is more likely to induce a response than endocrine therapy under these circumstances.
Confirming the diagnosis In general, a biopsy is indicated at the time of first suspected recurrence in women with a prior history of breast cancer. Solitary pulmonary nodules in particular require biopsy, since up to 50 percent represent new primary lung cancers, especially if there is a history of smoking Repeat biopsy may also permit a more precise characterization of relevant predictive factors. As an example, up to 20 percent of estrogen receptor (ER) measurements may be discordant between primary and metastatic lesions . In addition, the tumor molecular profile is becoming increasingly important in selecting therapies, such as trastuzumab for HER2-positive tumors
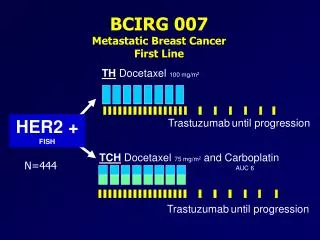
Endocrine therapy versus chemotherapy for HER2-positive disease Trastuzumab is the preferred initial agent for patients with HER2-positive tumors. For patients with relatively indolent disease, it is reasonable to try trastuzumab alone or trastuzumab plus endocrine therapy for a few months. Some patients may respond and be well palliated. An alternative for patients with symptomatic or rapidly progressive visceral metastases is combined therapy Amplified/overexpressed HER2 predicts for response to therapies that target HER2, such as the humanized monoclonal antibody trastuzumab (Herceptin) and the small molecule tyrosine kinase inhibitor lapatinib (Tykerb®)
These drugs are only effective in those patients whose tumors have high levels of HER2 overexpression (3+ by immunohistochemistry) or gene amplification (as detected by fluorescence in situ hybridization, FISH) of HER2 About 24 percent of IHC 2+ positive tumors have gene amplification by FISH, and these patients have the potential to respond to trastuzumab. some women with HER2-negative primary tumors acquire HER2 protein overexpression at recurrence
predictors of chemotherapy response The most consistent predictors of poor chemotherapy response are progression with prior chemotherapy for advanced disease, relapse within 12 months of completing adjuvant chemotherapy, poor performance status, and multiple disease sites, especially visceral involvement
bisphosphonate therapy in MBC Among women with lytic, and probably blastic, bone metastases, bisphosphonate therapy in combination with either endocrine therapy or chemotherapy prolongs the time to first skeletal complication and decreases the proportion of women who develop complications related to bone metastases The American Society of Clinical Oncology recommends intravenous pamidronate (90 mg over one to two hours every four weeks) in such patients
tumor marker Serial tumor marker assay can be particularly helpful in confirming a clinical suspicion of a change in the biologic course. CA 15-3 and CA 27.29 are well-characterized assays that detect circulating MUC-1 antigen in peripheral blood. (ASCO), monitoring selected patients with metastatic disease in the absence of readily measurable disease was the sole recommended use for circulating tumor markers including CA15-3, CA27.29, and CEA
tumor marker If the MUC-1 assay is elevated, there is no role for monitoring CEA, but if not, then serial CEA levels may be useful. Up to 20 percent of patients successfully treated with systemic therapy may experience a transient increase (marker "flare") during the first one or two months after treatment initiation, presumably due to release of antigen by cytolysis Patients with abnormal liver function may also have falsely elevated marker levels because they are cleared by the liver CA 15-3 levels may be aberrantly elevated in patients with vitamin B12 deficiency and megaloblastic anemia, as well as in patients with thalassemia or sickle cell disease
single agents & combination chemotherapy We suggest therapy with serial single agents rather than initial combination chemotherapy for patients with nonvisceral or slowly progressive visceral disease (G2B). For elderly women and those with a borderline performance status, single agent vinorelbine is a reasonable alternative to anthracyclines or a taxane
single agents & combination chemotherapy For selected, highly symptomatic patients and those with rapidly progressive visceral metastases, we suggest initial combination therapy rather than serial single agents because of the greater likelihood of an objective response There is no single regimen that has emerged as superior
high dose chemotherapy There is no proven benefit for high dose chemotherapy with hematopoietic stem cell support,
single agents & combination chemotherapy Due to the lack of survival and QOL benefit, we suggest serial single agents rather than combination chemotherapy for second, third, or fourth-line treatment for most patients with slowly progressive, asymptomatic disease (Grade 2B). For patients whose disease is rapidly progressive or symptomatic, the risks and benefits of combination therapy must be discussed with the patient, and treatment individualized.
circulating levels of the HER2 protein extracellular domain (ECD) Multiple studies have addressed whether circulating levels of the HER2 protein extracellular domain (ECD) can predict response to trastuzumab (or lapatinib) and is generally associated with a poorer prognosis
lapatinib Until further information is available, we suggest that lapatinib not be used as a first-line agent, even in patients with brain metastases
The role of surgery in metastatic breast cancer Patients with metastatic breast cancer are unlikely to be cured of their disease by any means. In the absence of curative treatment for the majority of patients, the goals of therapy typically shift from cure to palliation, focusing on symptom control, improved quality of life (QOL), and prolongation of survival. There are no randomized trials showing that resection of any metastatic site prolongs survival compared to systemic treatment alone.
The role of surgery in metastatic breast cancer At least three observational studies directly comparing outcomes of surgically treated patients with pulmonary or hepatic metastases with those receiving chemotherapy alone suggest a significant survival advantage for surgery However, caution is warranted in interpreting the results of comparative studies due to the selection bias that is inherent in such reports. Patients with significant comorbidities are rarely considered good operative candidates and are more often recommended for nonsurgical therapies. In addition, patients selected for surgery are often those who have better prognostic features or indolent biologic behavior (ie, good performance status, solitary metastases, long disease-free interval).
The role of surgery in metastatic breast cancer Most oncologists consider the presence of disease outside one organ to be a contraindication to metastatectomy, although there are exceptions to this general rule
The role of surgery in metastatic breast cancer Patients with a history of breast cancer and a new solitary pulmonary lesion should be strongly considered for resection, because of the possibility that this represents a potentially curable primary lung cancer.
The role of surgery in metastatic breast cancer Contraindications to hepatic resection include bilobar disease, hilar involvement, or insufficient liver function to permit resection.
The role of surgery in metastatic breast cancer Craniotomy should be considered for patients with a single accessible large or symptomatic brain metastasis. The role of surgery for patients with multiple brain metastases is controversial.