Download
1 / 62
680 likes | 1.17k Views
Chronic Obstructive Pulmonary Disease (COPD). Omer Alamoudi, MD, FRCP,FCCP,FACP Professor, consultant Pulmonologist dramoudi@yahoo.com. Definition of COPD. COPD is a chronic obstructive pulmonary disease that is characterized by airflow limitation that is not fully reversible.

E N D
Chronic Obstructive Pulmonary Disease (COPD) Omer Alamoudi, MD, FRCP,FCCP,FACP Professor, consultant Pulmonologist dramoudi@yahoo.com
Definition of COPD • COPD is a chronic obstructive pulmonary disease that is characterized byairflow limitation that is not fully reversible. • The airflow limitation is usually bothprogressive and associated with an abnormal inflammatoryresponse • COPD is a preventable and treatable disease
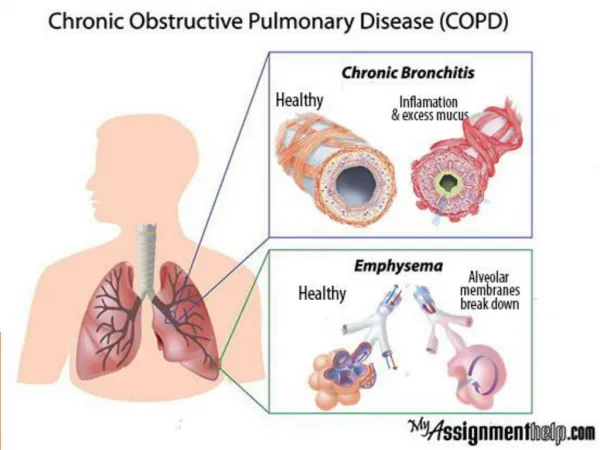
Chronic Obstructive Pulmonary disease (COPD) • Chronic bronchitis • Emphysema
COPD • Definitions • Chronic bronchitis: Cough and sputum production for at least 3 months in each of two consecutive years in albescence of other endobronchial disease such as bronchiectasis • Emphysema: overinflation of the distal airspaces with destruction of alveolar septa
Prevalence/Risk Factors Cigarette Smoking • Cigarette smoking is the primary cause of COPD. • Approximately 90% of COPD patients have a smoking history • The WHO estimates 1.1 billion smokers worldwide, increasing to 1.6 billion by 2025. • In low- and middle-income countries, rates are increasing at an alarming rate • .
Smoking Prevalence Among Doctors Country Male% Female% UK 8 5 USA 9 7 Germany 9 6 Korea 46 28 China 42 35 S. Arabia 38 15
2020 1990 Global Burden of Disease (1990–2020)
COPD Prevalence in KSA (Contd.) • According to one report released by the executive office of the GCC Health Ministers Council, Saudi Arabia is the world’s fourth largest importer of cigarettes. • During the year of 2004, the kingdom imported 41,000 tons of tobacco at a value of SR 1.45 billion.
Table 3. Ranking of the 10 most frequent diagnoses among hospitalized patients at KAUH Diagnosis No % Diabetes mellitus 570 10.5 Ischemic heart diseases 493 8.6 Bronchial asthma 311 5.8 Chronic liver disease 293 5.4 Congestive heart failure 203 3.8 Hypertension 153 2.8 Sickle cell anemia 141 2.6 COPD 132 2.4 Chronic renal failure 116 2.1 Cerebrovascular accident 108 2.0
Risk Factors for COPD Host Factors Genes (e.g. alpha1-antitrypsin deficiency) Hyperresponsiveness Exposure Tobacco smoke Occupational dusts and chemicals Infections Socioeconomic status
Risk Factors for COPD Nutrition Infections Socio-economic status Aging Populations
Pathogenesis of COPD NOXIOUS AGENT(tobacco smoke, pollutants, occupational agent) COPD Genetic factors Respiratory infection Other
Source: Peter J. Barnes, MD Pathogenesis of COPD Cigarette smoke Biomass particles Particulates Host factors Amplifying mechanisms LUNG INFLAMMATION Anti-oxidants Anti-proteinases Oxidative stress Proteinases Repair mechanisms COPD PATHOLOGY
Causes of Airflow Limitation • Irreversible • Fibrosis and narrowing of the airways • Loss of elastic recoil due to alveolar destruction • Destruction of alveolar support that maintains patency of small airways
Diagnosis of COPD • A clinical diagnosis of COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and/or a history of exposure to risk factors for the disease. • The diagnosis should be confirmed by spirometry. A post-bronchodilator FEV1/FVC < 0.70 confirms the presence of airflow limitation that is not fully reversible. • Comorbidities are common in COPD and should be actively identified.
Diagnosis of COPD EXPOSURE TO RISK FACTORS SYMPTOMS cough tobacco sputum occupation shortness of breath indoor/outdoor pollution è è è SPIROMETRY
Diagnosis of COPD • Signs • Hands • Flapping tremor, dilated veins, collapsing pulse, warm hands (CO2 retention) • Cyanosis, clubbing of the finger (ca lung) • Chest (signs of hyperinflation) • Barrel chest, use of accessory ms, decreased expansion, absence cardiac dullness, tracheal tug • Hyperesonant on percussion
Diagnosis of COPD • Sign of pulmonary HTN • Increased JVP, left parasternal heave, Loud P2, Hepatomegaly, Ascitis, lower limb edema • Fundus examination • Papilloedema • Extrapulmonary manifestation • Ms wasting
Diagnosis of COPD: Spirometry • Spirometry should be performed after the administration of an adequate dose of a short- acting inhaled bronchodilator to minimize variability. • A post-bronchodilator FEV1/FVC < 0.70 confirms the presence of airflow limitation that is not fully reversible.
Classification of COPD Severity by Spirometry Stage I: MildFEV1/FVC < 0.70 FEV1> 80% predicted Stage II: ModerateFEV1/FVC < 0.70 50% < FEV1 < 80% predicted Stage III: SevereFEV1/FVC < 0.70 30% < FEV1 < 50% predicted Stage IV: Very SevereFEV1/FVC < 0.70 FEV1 < 30% predicted or FEV1 < 50% predicted plus chronic respiratory failure
The Effect of Smoking on Lung Function FEV1 (% of value at age 25 y) Never smoked or notsusceptible to smoking 100 75 Smoked regularly andsusceptible to its effects 50 Stopped at 45 DISABILITY 25 Stopped at 65 DEATH 0 25 50 75 Age (y) Adapted from Fletcher & Peto 1977
Diagnosis of COPD • CBC WBC (increased with infection) Hb (secondary Polycthemia) • ESR Increased with infection malignancy
Diagnosis of AECOPD • Diagnosis of AECOPD was based on ATS criteria • Major • Increased dyspnea • Increased sputum production • Purulent sputum • Minor • Cough, wheeze, sore throat, and cold and nasal discharge
Diagnosis of AECOPD/sputum culture • Pathogens isolated during exacerbation • Bacterial • Moraxella catarrhalis • Pseudomonas • Haemophilus influenzae • Viral • Influenza • Atypical bacteria • Mycoplasma • Chlamydia
Differential Diagnosis: COPD and Asthma COPD ASTHMA • Onset early in life (often childhood) • Symptoms vary from day to day • Symptoms at night/early morning • Allergy, rhinitis, and/or eczema also present • Family history of asthma • Largely reversible airflow limitation • Onset in mid-life • Symptoms slowly progressive • Long smoking history • Dyspnea during exercise • Largely irreversible airflow • limitation
COPD and Co-Morbidities COPD patients are at increased risk for: • Myocardial infarction, angina • Osteoporosis • Respiratory infection • Depression • Diabetes • Lung cancer
Pulmonary Hypertension in COPD Chronic hypoxia Pulmonary vasoconstriction Muscularization Intimal hyperplasia Fibrosis Obliteration Pulmonary hypertension Cor pulmonale Edema Death Source: Peter J. Barnes, MD
Management of COPD Prevention • Smoking cessation:is the single most effective — and cost effective — intervention in most people to reduce the risk of developing COPD and stop its progression • Controlling pollution:Reduction of total personal exposure to tobacco smoke, occupational dusts and chemicals, and indoor and outdoor air pollutants are important goals to prevent the onset and progression of COPD.
Management of COPD Smoking cessation • Counseling delivered by physicians • Numerous effective pharmacotherapies for smoking cessation are available • Nicotine chewing gum, transcutaneous patches, nicotine inhalers or nasal spray • Buproprion (aminoketone) (reduce nicotine withdrawal symptoms) • Epilepsy, tremor, insomnia, tachycardia • Nortiptyline