Download
1 / 42
420 likes | 444 Views
Central nervous system. Guanghui Yu Radiology college. dura mater the outer layer arachnoid mater the middle layer pia mater the inner layer inseparable from the brain The cranial dura is formly adherent to the periosteum of skull bones

E N D
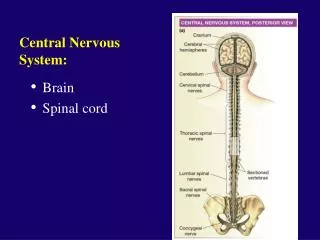
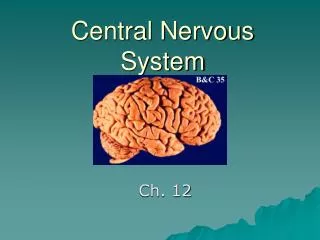
Central nervous system Guanghui Yu Radiology college
dura mater the outer layer arachnoid mater the middle layer pia mater the inner layer inseparable from the brain The cranial dura is formly adherent to the periosteum of skull bones The arachnoid mater is loosely adherent to the dura mater Between the arachnoid and the pia is the subarachnoid space Meninges
according to location Epidural Haematoma Subdural Haematoma subarachnoid haemorrhage intracerebral haematoma intraventricular haemorrhage Intracranial Hematoma
A haematoma is the inevitable consequence of the rupture of a blood vessel, either artery, vein or capillary The immediate consequence of the rupture is a haemorrhage The collection of blood outside the vessel forms the haematoma If the haemorrhage occurs within a fluid, such as CSF, the blood cannot collect and remains dispersed; for this reason the term used to describe the situation is subarachnoid haemorrhage , intraventricular haemorrhage Intracranial Hematoma
As for aetiology, the main causes of intracranial haemorrhage and haematoma are: trauma , hypertension, aneurysm rupture, arteriovenous malformation rupture, cerebral infarction(the blood usually oozes outside the ischemic vessel walls ) Less common causes are venous infarction, fungal or bacterial vasculitis with pseudoaneurysm formation , encephalitis and tumors
CT is the modality of choice located between the dura and the inner table of the skull tearing of the meningeal vessels ,especial middle meningeal artery the shape is usually biconvex may cross the midline associated with a skull fracture Epidural Haematoma
A small hyperdense lentiform collection of blood is seen over the left frontal convexity. Underneath a small focal haemorrhagic brain contusion is seen. An extracranial subgalean haematoma on the left side is also present.
CT is the examination of choice a collection of blood in the subdural space usually venous in origin , especial bridging veins mainly frontoparietal in location usually crescentic in shape Space-occupying effect Subdural Haematoma
mixed hyperdense hypodense collection with a crescentic shape is seen over the frontoparietal convexity on the left side. The lateral ventricle is displaced and there is a marked shift of the midline structures.
Coronal T1WI of a mixed density subacute subdural haematoma. The extracerebral fluid collection is mainly isointense with a small hyperintense component containing methaemoglobin. Marked mass effect with shift of the midline structures and the brainstem compression.
an acute extravasation of blood into the subarachnoid space CT scan clearly shows the hyperdensity of the subarachnoid spaces filled with blood usually following rupture of an aneurysm of the circle of Willis blood is cleared from the subarachnoid spaces within 1 week subarachnoid haemorrhage
interhemispheric cistern suprasellar cistern sulcus Intraventricular blood is also seen in the third and lateral ventricles
an intracerebral haematoma is considered acute within the first few days Subacute haematoma is usually between a week and a fortnight old after two weeks it is considered to be chronic intracerebral haematoma
The density or signal characteristics of the haematoma examined with CT or MR respectively vary with the age of the haematoma
acute Subacute haematoma
Acute A week later
intraventricular haemorrhage Haemorrhage in the basal ganglia area on the left ruptures into the lateral ventricle 5 hours after stroke
The main causes of infarction are atherosclerotic occlusion of large vessels, embolic occlusion of distal vessels, vasculitis and arterial spasm The common clinical presentation is stroke Ischemia is a prerequisite of infarction but may still be reversible; if permanent, irreversible damage to the nervous tissue results Cerebral Infarction
Different cell types have varying sensitivity to ischemia , neurones are the most sensitive to ischemia, followed by astrocytes, oligodendroglia, microglia and endothelial cells.
When a vessel is occluded, the entire supplied region does not become ischemic because efficient collateral circulation may develop very rapidly Some deep areas of the brain are border zones between the terminal capillary beds of the major cerebral arteries in the cortex and receive the lowest cerebral blood flow; these zones, called watershed areas, are the first to suffer ischemia and infarction during generalized systemic hypotension
When a patient presents with stroke or TIA (transient ischemic attack) or neurological signs indicating a possible vascular ischemic aetiology, a CT scan must be performed first If there is a discrepancy between the clinical status and the CT finding, it will be necessary to perform MRI, including diffusion and perfusion studies and MRA eventually followed by angiography, if intra-arterial thrombolysis is envisaged
The role of immediate CT is two-fold: diagnose or exclude any other cause , mainly haemorrhage ;and to recognize the extent of ischemia
Three phases may be identified: acute, subacute and chronic In the acute phase :about 60% of scans may be considered normal within the first few hours some subtle early signs may be detected : loss of grey-white matter interface obscuration of the lentiform nucleus hyperdensity of the middle cerebral artery
A rapid development of the picture may be seen after 6-8 hours with the development of cytotoxic oedema , the infarcted area becomes markedly hypodense with involvement of both grey and white matter , usually in a wedge-shaped area corresponding to the region of distribution of the occluded vessel about 15-20% of cases haemorrhagic foci may be detected after 24-48 hours
Axial CT without contrast, about two hours after stroke. Three arrows point at the hyperdensity of a thrombosed middle cerebral artery
Same patient: effacement of the sylvian fissure and mild temporoinsular hypodensity
Same patient: 24 hours later. Diffuse hypodensity of the right hemisphere , due to cytotoxic oedema Severe mass effect with subfalcial herniation and compression of the right lateral ventricle
(a) (b) (c) a. axial T2WI of a right temporoparietal ischemia (less than 2 hours). Almost no abnormalities are seen except a mild thickening of the cortex. b. Diffusion-weighted image. The cortical reduced diffusion is well seen. c. T2WI, 12 hours later. Cortical hyperintensity in the infarcted area, due to oedema
Intramedullary spinal cord tumor is atumor that arise from cells of the spinal cord and grow within it The most common histological types are: ependymomas (about 45%), astrocytomas (about 45%), haemangioblastomas (about 5%) and others (about 5%) Intramedullary spinal cord tumor
Diagnostically plain films of the spine are rarely positive CT is rarely useful MR is the gold standard today There are no specific signs that allow a definite histological diagnosis between the three main groups of ependymomas astrocytomas and haemangioblastomas
Usually a focal enlargement of the spinal cord is seen The lesion is hypointense in T1WI and hyperintense in T2WI Frequently the nodular component enhances There may be some edema above and below the tumor nodule about 30% of tumors an extensive intramedullary cyst is found
Frequently ependymomas are localized with a clear margin astrocytomas may be quite extensive Haemangioblastomas: Dilated draining veins are sometimes observed and the tumor nodule may be homogeneous and enhance strongly
Ependymoma midline sagittal T2WI of the dorsal spine: Focal widening of the spinal cord ,a mass is hyperintense on T2WI
(a) (b) (c) (d) a. Focal widening of the cord at the C4-C5-C6 levels with slight hypointensity. b. T2WI The tumor is hyperintense. c, d. T1WI following gadolinium injection. Marked inhomogeneous enhancement of the tumor. In (b) upward extension of the enhancement towards the medulla along the central canal is seen