Download
1 / 38
380 likes | 399 Views
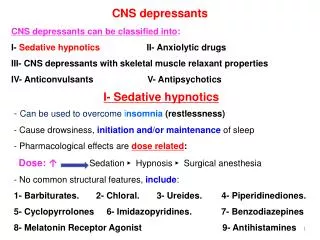
CNS Depressants. Prof. Faris Abachi College of Pharmacy University of Mosul. Classifications. 1- General Anesthesia 2- Sedative – Hypnotics 3- Anti – psychotic drugs 4- Anti – Consultants drugs. Mode of Action.

E N D
CNS Depressants Prof. Faris Abachi College of Pharmacy University of Mosul
Classifications 1- General Anesthesia 2- Sedative – Hypnotics 3- Anti – psychotic drugs 4- Anti – Consultants drugs. .
Mode of Action Positive modulation of the action of γ –amino butyric acid (GABA) at GABAA receptor .Except anti consultants has been associated with neuronal voltage - gated sodium channel block , leading to decrease neuronal excitation .
What are General Anesthetics? • A drug that brings about a reversible loss of consciousness. • These drugs are generally administered by an anesthesiologist in order to induce or maintain general anesthesia to facilitate surgery.
Background • General anesthesia was absent until the mid-1800’s • William Mortonadministered ether to a patient having a neck tumor removed at the Massachusetts General Hospital, Boston, in October 1846. • The discovery of the diethyl etheras general anesthesia was the result of a search for means of eliminating a patient’s pain perception and responses to painful stimuli. (CH3CH2)2O
HISTORY OF ANESTHESIAINHALATION AGENTS • Nitrous Oxide • 1799 Davy • 1824 Hickman • 1844 Wells • Ether • 1842 Long • 1847 Snow
InhalationAnesthetics Gasses or Vapors Usually Halogenated IntravenousAnesthetics Injections Anesthetics or induction agents Anesthetics divide into 2 classes:
Inhaled Anesthetics • Halothane • Enflurane • Isoflurane • Desflurane • Halogenated compounds: • Contain Fluorine and/or bromide • Simple, small molecules
Nomenclature • Halothane • is an inhalational general anesthetic. Its IUPAC name is 2-bromo-2-chloro-1,1,1-trifluoroethane.
Stages of Anesthesia • 1- Stage I :Cortical stage • 2- Stage II :Excitement • 3- Stage III :surgical Anesthesia • 4- Stage IV :Modularly Paralysis
Component of general anesthesia • 1-Uncinicousness ( Hypnosis ) • 2- Analgesia • 3- Muscles relaxants .
Routine Monitors ECG. BP. Oximetry (2 wavelengths , red and infrared) End Tidal CO2 . Temperature (axillary vs. core). FUTURE : Depth of anesthesia - BIS (Bispectral index EEG) -scale from 0 to 100 BIS > 65 deepen.
Physical and Chemical Properties of Inhaled Anesthetics • Although halogenations of hydrocarbons and ethers increase anesthetic potency, it also increase the potential for inducing cardiac arrhythmias in the following order F<Cl<Br.1 • Ethers that have an asymmetric halogenated carbon tend to be good anesthetics (such as Enflurane). • Halogenated methyl ethyl ethers (Enflurane and Isoflurane) are more stable, are more potent, and have better clinical profile than halogenated diethyl ethers. • fluorination decrease flammibity and increase stability of adjacent halogenated carbons. • Complete halogenations of alkane and ethers or full halogenations of end methyl groups decrease potency and enhances convulsant activity. Flurorthyl (CF3CH2OCH2CF3) is a potent convulsant, with a median effective dose (ED50) for convulsions in mice of 0.00122 atm. • The presence of double bonds tends to increase chemical reactivity and toxicity.
Intravenous Anesthetics • Used in combination with Inhaled anesthetics to: • Supplement general anesthesia • Maintain general anesthesia • Provide sedation • Control blood pressure • Protect the brain
Intravenous Anesthetics • Thiopental Sodium ( Ultrashort acting barbiturates), 3D-structure ;
Benzodiazepines • Alone cant produce surgical anesthesia, i.v. used to introduce anesthesia.Relaxant.
Uses of Benzodiazepines • Benzodiazepines generally share the same pharmacological properties, such as anxiolytic, sedative, hypnotic, skeletal muscle relaxant, amnesic and anticonvulsant (hypertension in combination with other anti hypertension medications).
Propofol ( Diprivan ) • It is a 2 , 6 diisopropylphenol (Emulsion ) • Used o inducion and maintenance of anesthesia . Has lipid / water P.C. The drug binds alloster ically o GABA A2
Ketamine Hydrochloride ( Ketalar) • ± 2- ( o-chlorophenyl) -2- methyl amino cyclohexanone HCI . ( racemic mixtures ) • Ketamine produces a sense of dissociation from events being experienced , followed by anesthesia , analgesia and sometimes amnesia.
Essential Components of Anesthesia • Analgesia- perception of pain eliminated • Hypnosis- unconsciousness • Depression of spinal motor reflexes • Muscle relation * These terms together emphasize the role of immobility and of insensibility!
Lipid Theory: based on the fact that anesthetic action is correlated with the oil/gas coefficients. The higher the solubility of anesthetics is in oil, the greater is the anesthetic potency. Meyer and Overton Correlations Irrelevant 2. Protein (Receptor) Theory: based on the fact that anesthetic potency is correlated with the ability of anesthetics to inhibit enzymes activity of a pure, soluble protein. Also, attempts to explain the GABAA receptor is a potential target of anesthetics acton. Hypotheses of General Anesthesia
Binding theory: Anesthetics bind to hydrophobic portion of the ion channel Other Theories included
Mechanism of Action UNKNOWN!! • Most Recent Studies: • General Anesthetics acts on the CNS by modifying the electrical activity of neurons at a molecular level by modifying functions of ION CHANNELS. • This may occur by anesthetic molecules binding directly to ion channels or by their disrupting the functions of molecules that maintain ion channels.
Cont on Mechanism • Scientists have cloned forms of receptors in the past decades, adding greatly to knowledge of the proteins involved in neuronal excitability. These include: • Voltage-gated ion channels, such as sodium, potassium, and calcium channels • Ligand-gated ion channel superfamily and • G protein-coupled receptors superfamily.
Pharmacokinetics of Inhaled Anesthetics • Amount that reaches the brain • Indicated by oil:gas ratio (lipid solubility) • Partial Pressure of anesthetics • 5% anesthetics = 38 mmHg • Solubility of gas into blood • The lower the blood:gas ratio, the more anesthetics will arrive at the brain • Cardiac Output • Increased CO= greater Induction time
Rate of Entry into the Brain: Influence of Blood and Lipid Solubility
Increase in Anesthetic Partial Pressure in Blood is Related to its Solubility
General Actions of Inhaled Anesthetics • Respiration • Depressed respiration and response to CO2 • Kidney • Depression of renal blood flow and urine output • Muscle • High enough concentrations will relax skeletal muscle
Cont’ • Cardiovascular System • Generalized reduction in arterial pressure and peripheral vascular resistance. Isoflurane maintains CO and coronary function better than other agents • Central Nervous System • Increased cerebral blood flow and decreased cerebral metabolism