Download
1 / 37
370 likes | 479 Views
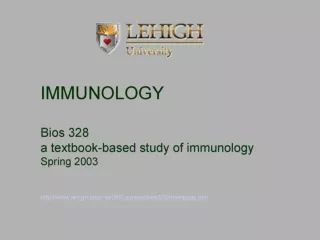
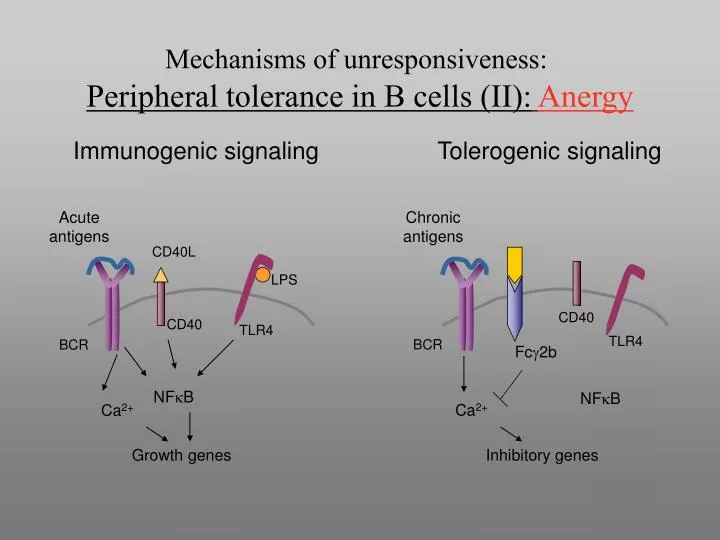
Acute antigens. CD40L. Chronic antigens. LPS. CD40. TLR4. BCR. CD40. NF k B. Ca 2+. TLR4. BCR. Fc g 2b. Growth genes. NF k B. Ca 2+. Inhibitory genes. Mechanisms of unresponsiveness: Peripheral tolerance in B cells (II): Anergy. Immunogenic signaling. Tolerogenic signaling.

E N D
Acute antigens CD40L Chronic antigens LPS CD40 TLR4 BCR CD40 NFkB Ca2+ TLR4 BCR Fcg2b Growth genes NFkB Ca2+ Inhibitory genes Mechanisms of unresponsiveness:Peripheral tolerance in B cells (II):Anergy Immunogenic signaling Tolerogenic signaling
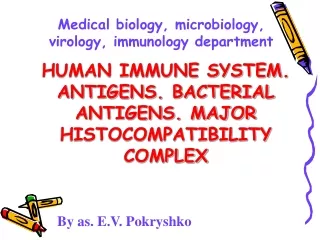
The two-signal requirement for T cell activation Microbial antigen presented by APC TCR MHC Signal 1 APC Signal 2 B7 Costimulatory Receptor (CD28)
CD28 B7 CD28 The role of co-stimulation in T cell activation Antigen recognition T cell response Resting APC: (costimulator- deficient) No response Activation of APC Innate immune response Activated APC: increased expression of costimulators, secretion of cytokines T cell proliferation And differentiation
B7 CTLA-4 B7 CD28 Regulation of T cell homeostasis during immune responses Anergy T cell expansion Magnitude of T cell response Apoptosis Activated T cells express CTLA-4 Surviving memory cells Activated T cells are deprived of antigen and other stimuli T cell activation Time after antigen exposure
Suppressor T cells Role of cytokines in suppression of cell-mediated immune responses Antigen recognition T cell proliferation and differentiation Effector functions of T cells IL-12 Effector T cells (TH1) Activated macrophages APC Naïve T cell IFN- Cytokines produced by suppressor T cells IL-10 inhibits Functions of APCs: IL-12 secretion, B7 expression TGF- inhibits T cell proliferation IL-4 inhibits action of IFN- IL-10, TGF- inhibit macrophage activation
Immunosurveillance: Tumors which Evolve in Lymphocyte Deficient Hosts are Rejected in WT Mice 100% RAG-/- WT Tumor (Sarcoma) Incidence is Increased in MCA-treated Lymphocyte Deficient Mice Tumor Incidence 0% Tumor: WT origin RAG-/- origin Tumors which developed in RAG-/- hosts are REJECTED in WT Recipients Tumor Size Host: RAG-/- WT
Immune Surveillance: Tumor Cell Expression of IFNg Receptor is Required for Lymphocyte-Mediated Tumor Rejection 100% IFNgR-/- WT Tumor Incidence after MCA Treatment 0% -------------------Transplanted tumor------------------------------------- IFNgR -/- transfected with IFNgR IFNgR -/- transfected with IFNgR WT IFNgR-/- Tumor Size Host: WT WT WT RAG-/-
IMMUNE RECOGNITION Cross-Priming: Induction of Anti-tumor T cell response Provide TH1 or 2 Help for B cell Ab Responses IL-2 CTL CD28 CD8 TCR CD4 CD4 TH1 TCR CD40L ClassI +peptide Class II + peptide B7 Tumor Cell CD40 APC Dendritic Cell Ag Processing/ presentation of peptides Endocytosis/ phagocytosis
Effector Mechanisms CD8 CTL Can Recognize Class I –peptide Complex and Induce Tumor Lysis and Apoptosis CD8 CTL Granule exocytosis: Perforin/granzyme TCR Class I + peptide Fas - FasL Tumor Cell
Effector Mechanisms Macrophages are Cell-Mediated Effectors TNF (+ other TNF-family members) NO, O2•, proteases CD4 CD4 TH1 TCR CD40L Class II + peptide Cytokine- Mediated Activation IFN-g GM-CSF TNF CD40 Macrophage
Effector Mechanisms Antibody Bound Targets Induce Myeloid Cell Tumor Cyto- toxicity Through Fc Receptors +/or Complement Receptors Y Y Y Y Tumor Cell ADCC, phagocytosis, release of inflammatory mediators (NO, O2•, proteases, TNF, etc.,) Y C3b CR1 FcR Macrophage
Tumor Evasion: Two Separate Problems • Tumor antigens are not recognized by immune response-poorly immunogenic (Immunologically ignorant). • Tumors are resistant to or inhibit immune cytotoxic responses. (active suppression—either dampen “priming” or avoid/inhibit/resist effector cell function).
Strategies for induction of anti-tumor Immune Responses -Passive- • Adoptive transfer of T cells:Antigenic specific T cell clones-requires HLA-restricted “customized” therapy or cytokine-enhanced antigen-non-specific T cells (LAK cells). Has worked for EBV lymphoproliferative disorders. • Monoclonal and engineered antibodies: 1. Humanized/chimeric mAbs: Herceptin (anti-HER2), Rituxan (anti-CD20), anti-idiotype (custom therapy), anti-EGFR (Erbitux), CAMPATH (anti-CD52), anti-VEGF (targets neovasculature, Avastin). 2. Immune conjugates (“smart bombs”) mAb-toxin (Mylotarg: anti-CD33 calicheamicin), mAb-chemo, mAb-isotope (anti-CD20 Zevalin and Bexxar).
Model of Innate Recognition and Initiation of the Adaptive Antitumor Immune Response Amplification of innate and link to adaptive response “danger”= invasion (inflam. response) + “stress” ligands of NKG2D Apoptosis provides antigen delivery to DCs Elimination by adaptive response
Rituxan (anti-CD20) High response rate in B cell lymphoma (>70%). Synergy with chemotherapy or XRT. Recognizes B cell marker regulating B cell activation. Induces growth arrest/apoptosis in vitro. Herceptin (anti-HER2) Lower response rate in breast cancer (15%). Synergy with chemo (60%) or XRT. Recognizes EGF-like receptor regulating cellular proliferation (ERBB2). Induces growth arrest/apoptosis in vitro. Monoclonal Antibody Therapeutics in Cancer
Immunopathology of MS Perivascular infiltrate of CD4+ T cells and APCs CD4+ T cells and dying, MHC class II + oligodendrocyte Myelin naked axon (plaque) Oligodendrocytes
Immunopathophysiology of Diabetes Dendritic cell/ APC Activated TH1 CD4+ T Cell CD2 CD4+ Cell (TH0 ) IL-12 DR3, DR4,,DQ8/gad, insulin peptide CD40L a,b, TCR IFN-g CD40 IL-4 Macrophage/dendritic cell CD4+ Cell (TH2 ) Fc R FasL perforin CD40L IL-1, TNF, LT, NO, PGE-2 CD8+ CTL IL-4 CD40L ?anti-insulin, GAD ab anti-Mog B Cell b cell death b islet cells ?Antibody mediated injury
Pathophysiology of Scleroderma DR/peptide TCRa,b CD4+ T Cell CD4 IL-1, TNF, TGF-b Dermal fibroblast IL-2 TCR a,b IFN-g IL-2R CD4 Activated CD4+ T Cell Fibroblast proliferation IL-2, IL-4, IL-5, IL-6 PGE2, collagen Fibrosis SmIg SmIg B Cell Anti-scl 70, Ro, La and RFs MHC class II Plasma Cell
CD4+ T cell Driving force Autoreactive to self peptides Autoreactive B cells IgG autoantibody Production Autoantibody-mediated Disease SLE pathogenesis Environmental triggers (drugs, microbes ?) Genetic susceptibility: Complex polygenic Genes Involved: MHC class II Complement deficiency Multiple non-MHC (unknown) X-chromosomal (unknown) Self-antigen driven Other genetic influences ?
Two major mechanisms of antibody-mediated tissue injury operating in SLE
Disease: Vasculitis Glomerulitis Arthritis Pleuritis Pericarditis Dermatitis Serum Sickness develops after injection of soluble foreign antigens
Why do SLE patients make autoantibodies? (1) Anti-self immunity: abrogation of self tolerance SLE might be the result of insufficient elimination of autoreactive T cell clones in the thymus or periphery. This might result in such autoreactive T cells being released into the peripheral circulation and causing the autoimmune features of the disease (2) Hidden antigens The nuclear and cytoplasmic antigens that are associated with autoimmunity are not commonly exposed to the immune system. If such antigens (dsDNA, for example) are liberated during cellular turnover, they may incite an immune response. Thereafter, further release of such antigens might form the nidus for IC
Why do SLE patients make autoantibodies? (3) Cross reactivity SLE might be a disease caused by an unknown pathogen such as a virus or a bacterium. The interaction of pathogen derived peptides with a susceptible HLA haplotype may elicit "autoimmune" diseases by activating pathogenic T cells. Such a pathogen has not been identified in SLE, but no feature of the disease suggests that this could not be the etiology. (4) Abnormal regulation: failure of suppression SLE might arise as a consequence of abnormalities in regulatory CD4+ or CD8+ T cells.
Evidence that T cells are important in the development of SLE • The pathogenic anti-DNA antibodies in SLE are high affinity IgG molecules. Because it is known that class switching to IgG as well as somatic mutation and affinity maturation requires T cells we infer that anti-DNA antibody-producing B cells are expanded in SLE by a process that mimics the normal CD4+ T cell-dependent responses, involving common mechanisms of somatic mutation, affinity maturation, and IgM to IgG class switching. • The MHC class II restriction and the known association of DR2 and DR3 with susceptibility to SLE also strongly point to a predominant role CD4+ T cells in the induction of autoimmunity in SLE. • Finally, animal models of SLE are effectively treated with molecules which block key functions of CD4+ T cells.
Induction of CD4+ TH1 mediated autoimmunity: A paradigm for the pathogenesis of rheumatoid arthritis, multiple sclerosis and type I diabetes (1) expansion of CD4+, autoreactive TH1 cells specific for autoantigens (2) migration and infiltration of these self reactive CD4+ TH1 cells into tissues and induction of inflammation and autoimmunity (3) induction of regulatory cells and cytokines which control the growth and activation of the pathogenic autoreactive CD4+ T cells MHC/self-peptide CD4 CD4 MHC/Vb TCR Vbx TCR Vbx APC CD4+ Vbx T cell Activated autoreactive CD4+ TCR Vbx TH1 cell
T-Macrophage Interactions Induce Synovial Cell Proliferation and Activation DR4/peptide CD2 a,b, TCR Fc Receptor CD4+ TH1 Cell CD4 Rheumatoid factor (RF) CD40L Macrophage IL-1, TNF, TGFb BONE RESORBTION CD40 inflammation Synthesis of PGE-2, Collagenase, IL-1 Synovial Cell Proliferation
Inflammation Immunopathophysiology of Rheumatoid Arthritis Dendritic cell/ APC CD2 Activated TH1 CD4+ T Cell CD4+ Cell (TH0 ) IL-12 DR4/RA peptide CD40L a,b, TCR IFN-g CD40 IL-4 RF Macrophage Sm Ig CD4+ Cell (TH2 ) Fc R PGE-2, collagenase chemokines RA antigen IL-1, TNF, TGFb B Cell Osteoclast activation Synovial fibroblast Endothelial cell Rheumatoid factor (RF) Plasma Cell (1) Synthesis of PGE-2, Collagenase, IL-1 (2) synovial cell proliferation Bone and cartilage destruction hypothalamus Vasculitis Fever
Rheumatoid Factors and Immune Complexes Augment the Activation of Macrophages DR4/peptide CD2 a,b, TCR Fc Receptor CD4+ TH1 Cell Rheumatoid factor (RF) or immune complexes CD4 CD40L Macrophage IFN-g IL-1 CD40 Increased synthesis of IL-1, TNF, TGF-b, IL-6, PGE2 and Collagenase Rheumatoid factor (RF) Activated Macrophage
TNF, IL-1 and RANK-L activate osteoclasts to induce bone resorption CD2 a,b, TCR Activated CD4+ T Cell Mf/dendritic cell RANK-L CD40 TNF CD40 Soluble RANK-L B7 MHC class II TNFR Soluble RANK Receptor (osteoprotegerin) RANK TNF IL-1 PGE2 Precursor Osteoclast Bone Resorption Activated Osteoclast
Mechanisms of action of drugs used to treat RA (a) Block T-APC interaction antibodies to MHC class II, CD4 or the TCR (b) Decrease T cell activation cyclosporine, anti-CD3, anti-CD28, anti-CD80 (B7), anti-CD40L, CTLA-4 agonist (e) Inhibit products of T/macrophages NSAIDs, TNF receptor inhibitors, IL-1 receptor inhibitors (c) Prevent T cell, B cell or synovial cell proliferation Methotrexate, immuran, cytoxan (d) Inhibit T cell or APC function steroids, gold, penicillamine
Spondyloarthritis Diseases 2. Genetic:- Susceptibility to develop disease is associated with inheritance of certain MHC class I alleles, notably HLA-B27 3. Pathogenesis:- CD8 T cells are centrally implicated while CD4 T cells or B cells are not essential as shown by MHC class I HLA associations, plus: • Occur at increased prevalence in those with advanced AIDS • No Autoantibodies “Seronegative” • CD8 T cells activated, clonally expanded and sometimes show antigen drive in sites of inflammation
Spondylitis Diseases • Ankylosing spondylitis • Reiter’s syndrome / reactive arthritis • Psoriatic arthritis • Undifferentiated spondyloarthritis • Enteropathic arthritis (ulcerative colitis, regional enteritis)
Spondyloarthritis Diseases 2. Genetic:- Susceptibility to develop disease is associated with inheritance of certain MHC class I alleles, notably HLA-B27 3. Pathogenesis:- CD8 T cells are centrally implicated while CD4 T cells or B cells are not essential as shown by MHC class I HLA associations, plus: • Occur at increased prevalence in those with advanced AIDS • No Autoantibodies “Seronegative” • CD8 T cells activated, clonally expanded and sometimes show antigen drive in sites of inflammation
Spondylitis Diseases • Ankylosing spondylitis • Reiter’s syndrome / reactive arthritis • Psoriatic arthritis • Undifferentiated spondyloarthritis • Enteropathic arthritis (ulcerative colitis, regional enteritis)
Reiter’s syndrome-Reactive arthritis -Mechanism Activation Disruption of “tolerance” of autoreactive CD8 T cells likely occurs through a combination of mechanisms: • Molecular mimicry - Older theory…T cell clones involved in attack on microorganisms expand and initiate attack on cells expressing target proteins that contain peptides that mimic the amino acid sequence found in the microorganisms • Provision of co-stimulatory signals by activated dendritic cells and macrophages in initial immune response to infection disrupts anergic or unreactive state of T cells • CD8 T cells express NK and other receptors that foster the activation of these cells by “danger” signals recognized by innate immune system receptors
CD8 -cell T CD8 T -cell Activation Cognitive and Clonal Expansion Recognition TCR Antigenic Peptide Self CD4 and CD8 Synovial or T Cell Recruitment Angiogenesis endon Fibroblast Synoviocyte Proliferation and Alteration in Gene Lining & Infiltrating Expression Monocyte / macrophage Activation Periosteal new bone formation Fibroblast Activation Inflammation, Destruction & Fibrosis Rx Methotrexate MHC class I Molecule T Rx TNF-a blockers