Download
1 / 56
640 likes | 900 Views
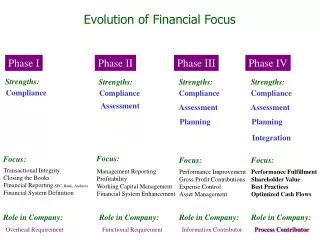
Phase I Trial Designs. Jud Blatchford, PhD Colorado School of Public Health January 30 th , 2013. Table of Contents. Orientation Introduction Components of a Phase I Trial Phase I Trial Designs Rule-Based Designs Statistical Designs References. Orientation. Orientation.

E N D
Phase I Trial Designs Jud Blatchford, PhD Colorado School of Public Health January 30th, 2013
Table of Contents • Orientation • Introduction • Components of a Phase I Trial • Phase I Trial Designs • Rule-Based Designs • Statistical Designs • References Phase I Trial Designs
Orientation Phase I Trial Designs
Orientation • Features of a Clinical Trial (CT) • Study of human beings • Prospective • Uses an intervention (i.e. changes some aspect of the subjects) • Protects the safety of the subjects • Follows an approved protocol Phase I Trial Designs
Orientation • Phases of Clinical Trials • Phase I – First time an experimental drug or treatment is tested in humans to examine how well the drug is tolerated • Phase II – Trials designed to examine if the drug or treatment has a biological treatment effect • Phase III – Trials designed to assess the treatment effect on a clinically meaningful endpoint • Phase IV – Post-marketing studies to gain additional information regarding the safety of the drug or treatment Phase I Trial Designs
Orientation • Components of Study Design • Rationale – Establishing a legitimate reason for the study • Design – Detailed description of what treatments will be administered, including a timeline of administration • Subjects – Determining the group to be studied and how they will be assigned to treatment groups • Data – Outcome measure(s), obtaining data, and QA • Sample Size Justification – Ensuring the study will be able to answer the scientific question with adequate power • Study Closure – Archiving study data, analysis files Phase I Trial Designs
Introduction Phase I Trial Designs
Introduction • Phase I Clinical Trials • An experimental drug, treatment, chemotherapeutic agent, cytotoxic agent, is studied—hereafter referred to as “drug” • Primary Goal: Safety • Investigate whether the new drug or combination of drugs can be administered safely to subjects • Investigate optimal dosing and administration of drug • Secondary Goal: Efficacy • Offer a treatment option to subjects who have failed other treatment regimens Phase I Trial Designs
Introduction • Underlying Assumptions • The drug kills both cancer cells and other cells • The effect is dose-dependent, therefore: • The efficacy of the drug increases with the dose • The toxicity of the drug increases with the dose • Logically, it would be optimal to give the subjects the highest dose of a drug that can be administered without unacceptable toxicity • Fundamental Question: What is this dose? Phase I Trial Designs
Maximum Tolerated Dose (MTD) • Definition of MTD: • The highest dose without observing an unacceptable rate of toxicity • Aliases: • Recommended Phase 2 Dose (RP2D) • Phase 2 Recommended Dose (P2RD) Phase I Trial Designs
Components of a Phase I Trial Phase I Trial Designs
Components of a Phase I Trial • Definition of a Dose-Limiting Toxicity (DLT) • Clarify time-frame for experiencing a DLT • Dose Levels • How many dose levels will be tested? • What will the smallest dose be? • What will the starting dose be? • Subjects • How many subjects will be tested? • Will single subjects or cohorts be tested at each dose? • What dose-escalation scheme will be employed? Phase I Trial Designs
Definition of a DLT • DLTs are typically defined using the National Cancer Institute’s (NCI) Common Terminology Criteria for Adverse Events (CTCAE). • DLTs are often grade ≥ 3 non-hematological and grade ≥ 4 hematological toxicities, which are definitely, probably, or possibly related to the drug. • CTCAE Grades • 0 – No AE • 1 – Mild • 2 – Moderate • 3 – Severe • 4 – Life threatening • 5 – Death • Degrees of Related • Unrelated • Unlikely • Possibly • Probably • Definitely Phase I Trial Designs
Definition of a DLT • The length of observation within which a DLT occurrence is “counted” should be explicitly stated in the protocol • Typical lengths used are the first cycle of chemotherapy (often 3 weeks) • Weight the trade-off between observation time for a DLT and efficiency in enrolling subjects Phase I Trial Designs
Choosing the Starting Dose • Goals: • Dose high enough to have chance of efficacy • Dose low enough to avoid a DLT • Use data from animal pre-clinical studies • Scale dose by body surface area (mg/m2) • Studies that aren’t “first-in-human” studies may be informed from previous studies using the same drug Phase I Trial Designs
Choosing the Starting Dose • Choices Used: • First find dose that is lethal in 10% of mice (LD10) • Standard starting dose was 10% of this dose (MELD10), if no grade 4+ AEs observed in other species (rats, dogs, etc.) • Find the highest dose for which the most sensitive animals investigated had no AEs • Starting dose is 1/3 of this level (scaled) • Find the minimal dose for which any toxicity is seen (TDL) • Starting dose is 1/3 of the TDL Phase I Trial Designs
Choosing the Number of Dose Levels • Testing more dose levels to accurately estimate the MTD creates a more cumbersome trial, and may require more subjects • Common number of levels is 4 to 7 • Observed number has ranged from 3 to 14 Phase I Trial Designs
Choosing the Dose Levels • Desire to progress through possible doses in a quick (e.g. exponential) manner • Ethical considerations should guide the dose escalation scheme used • Linear sequence of numbers may be inefficient • 20, 40, 60, 80, 100, 120, 140, … • Famous sequence of increasing numbers: • 1, 1, 2, 3, 5, 8, 13, 21, 34, 55, 89, 144, 233, 377, 610, 987, … Phase I Trial Designs
The Fibonacci Sequence Phase I Trial Designs
The Golden Ratio Phase I Trial Designs
The Golden Ratio Phase I Trial Designs
Modified Fibonacci Dose Escalation (MFDE) Phase I Trial Designs
Ethical Considerations • Approach the MTD from below (under-estimates MTD) • Bracketing the MTD is unbiased and more efficient • Expected efficacy is minimal • Historical response rate is 11%; temp. stable rate is 34% • 40% expect a cure • Subjects suffer significant toxicity • Rate of grade 4 toxicity is 14%; death rate is 0.5% • What subjects are told is very important Phase I Trial Designs
Phase I Trial Designs Phase I Trial Designs
Rule-Based Designs • Traditional Escalation Rule • Variations of the Traditional Escalation Rule • Best of 5 Rule • Up-and-Down Designs • 2-Stage Designs Phase I Trial Designs
Traditional Escalation Rule (TER) 3 subjects receive dose di 1 DLT 0 DLTs 2 or 3 DLTs 3 more subjects at dose di Escalate - 3 subjects receive dose di+1 Stop escalation De-escalate to di-1 0 DLTs (1/6 with DLT) 1—3 DLTs (≥ 2/6 with DLT) Escalate - 3 subjects receive dose di+1 Stop escalation De-escalate to di-1 De-escalate until a level is reached where at least 6 subjects are treated and at most 1 DLT occurs. MTD is the highest dose where at least 6 subjects were treated with at most 1 DLT. Phase I Trial Designs
Evaluating the TER Benefits Criticisms Many subjects treated at low, ineffective doses At least 2 subjects treated at level above MTD The true MTD is underestimated • Conservative escalation • Ease of implementation • Rules regarding dose assignment are clear • Statistical models not fit after each subject • Design is robust • Will arrive at reasonable estimate of MTD Phase I Trial Designs
Variations to TER • After escalation stops, fill out all lower levels until at least 6 subjects are treated at each level • Treat subjects at a dose level between the level where escalation stopped and the next lower level Phase I Trial Designs
Best of 5 Rule 3 subjects receive dose di 1 or 2 DLTs 3 DLTs 0 DLTs 1 more at dose di Stop escalation Escalate to dose di+1 1/4 with DLT 2/4 with DLTs 3/4 with DLTs Escalate to dose di+1 1 more at dose di Stop escalation 2/5 with DLTs 3/5 with DLTs Stop escalation Escalate to dose di+1 MTD is the dose prior to the dose on which escalation stopped. Phase I Trial Designs
Up-and-Down Design (UaD) 1 subject receives dose di 0 DLT 1 DLT Escalate to dose di+1 De-escalate to di-1 Perform UaD for a pre-specified number of subjects (j). MTD is the dose that would be assigned to the j+1st subject. Phase I Trial Designs
Storer’s C Design (UaD-C) 1 subject receives dose di 0 DLT 1 DLT If 2 consecutive subjects with 0 DLT, escalate to dose di+1; else give dose di De-escalate to di-1 Perform UaD for a pre-specified number of subjects (j). MTD is the dose that would be assigned to the j+1st subject. Phase I Trial Designs
Storer’s Two-Stage BC Design (UaD-BC) 1 subject receives dose di Stage 1 0 DLT 1 DLT De-escalate to di-1 Escalate to dose di+1 1 subject receives dose di-1 Stage 2 0 DLT 1 DLT De-escalate to di-2 If 2 consecutive subjects with 0 DLT, escalate to dose di; else give dose di-1 Perform UaD for a pre-specified number of subjects (j). MTD is the dose that would be assigned to the j+1st subject. Phase I Trial Designs
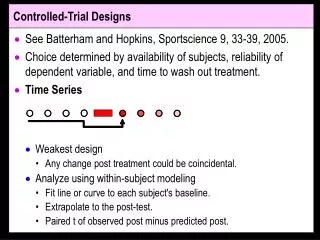
Accelerated Titration Designs Extension by Simon of Storer’s work Design 1: TER Designs 2—4 Stage 1: Single subjects until first DLT or second grade 2 AE Stage 2: TER Design 2: Toxicities observed in first cycle only Design 3: Toxicities may be observed in any cycle Design 4: Same as 3 except escalation factor is 2.0 Phase I Trial Designs
Statistical Designs Dose escalation guided by a statistical model of the relationship between dose and toxic response • Continual Reassessment Method • Modifications to the CRM • 2-Stage CRM Designs • TITE-CRM Phase I Trial Designs
Continual Reassessment Method (CRM) • First proposed by O’Quigley in 1990 • Subjects are enrolled individually • A dose-toxicity function is assumed • f(d | α) = Pr{DLT | α} • After each patient completes observation, the estimate of α is updated • Strategy is to assign the dose closest to the estimated MTD to each subject Phase I Trial Designs
Considerations for the CRM • Number of dose levels • Initial estimates of toxicity rates at each dose level • Target rate of DLT (θ) • Dose-toxicity function • Escalation restrictions • Number of subjects to be treated Phase I Trial Designs
Considerations Number of Dose Levels Initial Estimates of Toxicity The estimates should bound the target rate (θ) The CRM is not robust when doses tested do not induce toxicity • Typically between 3 and 8 • In general, as the number of dose levels in the trial increases, the number of subjects needed to accurately estimate the MTD will increase Phase I Trial Designs
Choosing a Dose-Response Function Logistic Function Logistic Regression Let p = Pr{DLT} Solving for p we have: One-parameter model: Phase I Trial Designs
Choosing a Dose-Response Function Hyperbolic Tangent Function Scaled Tanh Function Pr{DLT} = Phase I Trial Designs
Choosing a Dose-Response Function CDF of Normal Distribution P{DLT} Phase I Trial Designs
The Method of CRM • Dose-toxicity function and θ are chosen a-priori • Function is re-fit (i.e. new estimate of α is obtained) after each subject’s observed toxicity • New function is determined from the a-priori function and the vector of observed toxicities • Curve shifts to the right without toxicity; left with toxicity • Next subject is treated at the dose level whose Pr{DLT} is closest to θ Phase I Trial Designs
Distributions of DLT Occurrence By Dose Priors for Subject 1 Priors for Subject 26 Separation between dose levels becoming clearer • High degree of overlap of probabilities between doses Phase I Trial Designs
Evaluating the CRM Benefits Criticisms Starting dose is too high Dose escalation is too aggressive Trial length is too long • Few subjects are treated at low, ineffective doses • Subjects are treated at doses believed at the time to be the most efficacious, yet safe Phase I Trial Designs
Modified CRM • Start at the lowest dose level under consideration • Enroll two or three subjects at each cohort • Constrain dose escalation to increase by at most one dose level Phase I Trial Designs
“Practical” CRM • Proposed by Piantadosi • Based on pre-clinical toxicity data: • Choose dose that would produce low (10%) rate of DLT • Choose dose that would produce high (90%) rate of DLT • Estimate dose/toxicity curve that fits these 2 points • Use the dose/toxicity curve to find dose for θ • Treat three subjects at this level, then re-estimate the dose-toxicity curve, dose for θ, and tx 3 more • Repeat until target dose changes by < 10% Phase I Trial Designs
2-Stage CRM Designs • Stage 1: TER • “2 + 2” is a more common first stage than “3 + 3” • Continue until first toxicity is observed • Stage 2: CRM • After first toxicity, fit the dose-response curve using the toxicity data accrued thus far • Choose dose for next cohort of 2 as dose with estimated rate of DLT closest to θ Phase I Trial Designs
Time-to-Event CRM (TITE-CRM) • Builds on the CRM described thus far • Uses information from subjects accrued, even if they haven’t finished observation period • Subjects with DLT are given full weight • Subjects without DLT are given weight t/T. • Allows subjects to be enrolled without waiting for prior cohorts to finish • Benefits studies with delayed toxicity (e.g. radiation studies) Phase I Trial Designs
Example of a TITE-CRM Trial • Subject accrual is instantaneous • The majority of doses administered are near MTD Phase I Trial Designs
Additional TITE-CRM Considerations • Choice of weight function • Uniform toxicities may use a linear function • Expecting late toxicities may use a convex function • Expecting early toxicities may use a concave function • Setting a Margin (i.e. upper limit) on toxicity • If θ = 0.20 and Margin = 0.05, dose for next subject will be dose closest to 0.20 and not greater than 0.25 • Determine cumulative time exposure (B) before allowing escalation (e.g. B = 2) Phase I Trial Designs
Design Comparisons • Fitting a model to the data will improve the accuracy of the MTD found by rule-based designs • Model-guided designs only perform well if assumptions are met (θ in range of doses tested) • Conflicting results when designs compared • Few comparisons made on “level playing field” • Both rule-based and model-guided designs are in common use, for good reason Phase I Trial Designs