Download
1 / 1
10 likes | 146 Views
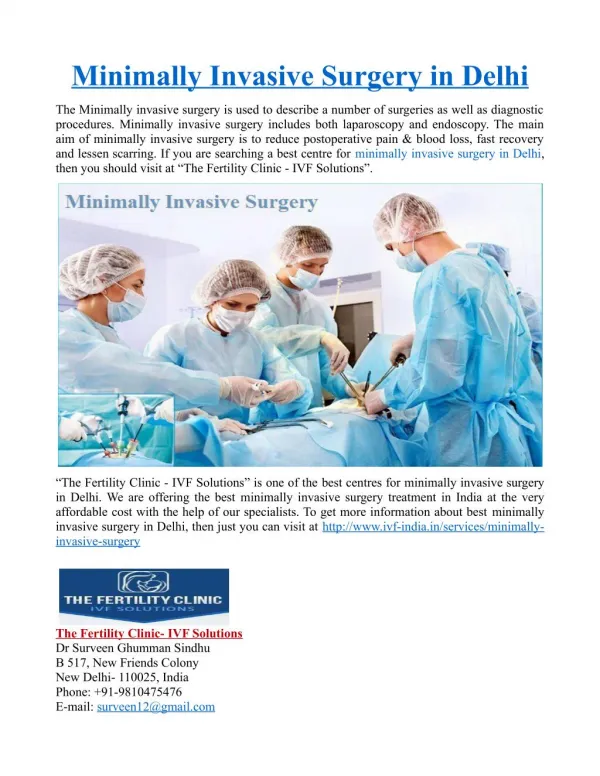
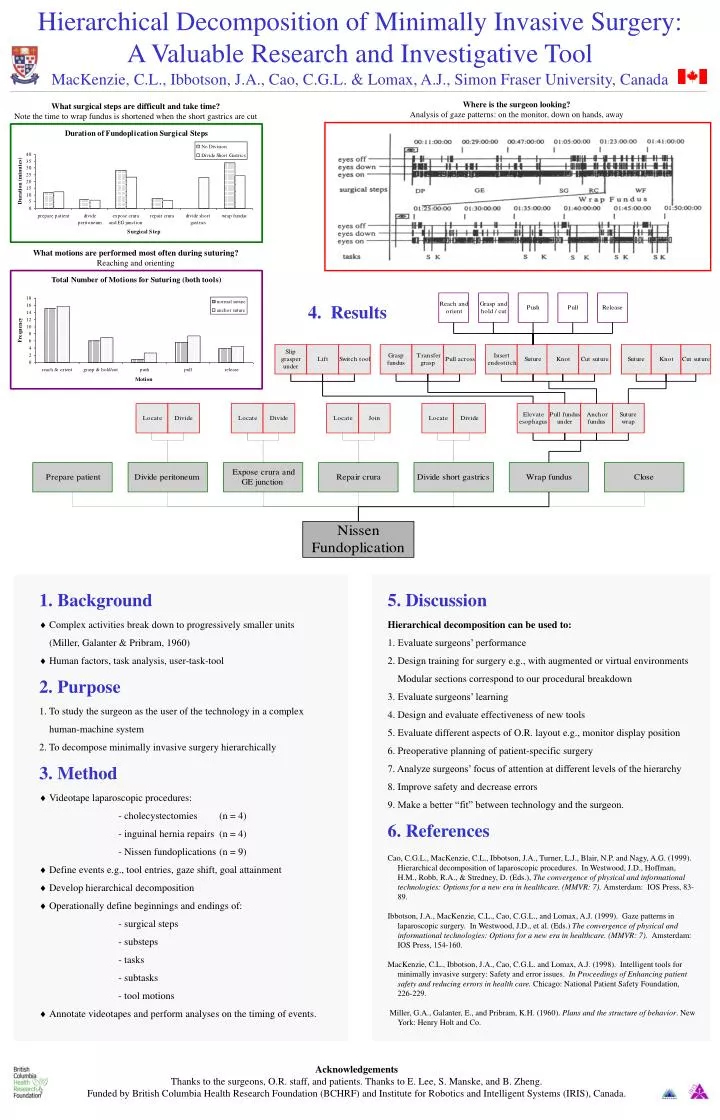
Hierarchical Decomposition of Minimally Invasive Surgery: A Valuable Research and Investigative Tool MacKenzie, C.L., Ibbotson, J.A., Cao, C.G.L. & Lomax, A.J., Simon Fraser University, Canada. Where is the surgeon looking? Analysis of gaze patterns: on the monitor, down on hands, away.

E N D
Hierarchical Decomposition of Minimally Invasive Surgery: A Valuable Research and Investigative Tool MacKenzie, C.L., Ibbotson, J.A., Cao, C.G.L. & Lomax, A.J., Simon Fraser University, Canada Where is the surgeon looking?Analysis of gaze patterns: on the monitor, down on hands, away What surgical steps are difficult and take time?Note the time to wrap fundus is shortened when the short gastrics are cut What motions are performed most often during suturing?Reaching and orienting 4. Results • 1. Background • Complex activities break down to progressively smaller units (Miller, Galanter & Pribram, 1960) • Human factors, task analysis, user-task-tool • 2. Purpose • 1. To study the surgeon as the user of the technology in a complex • human-machine system • 2. To decompose minimally invasive surgery hierarchically • 3. Method • Videotape laparoscopic procedures: • - cholecystectomies (n = 4) • - inguinal hernia repairs (n = 4) • - Nissen fundoplications (n = 9) • Define events e.g., tool entries, gaze shift, goal attainment • Develop hierarchical decomposition • Operationally define beginnings and endings of: - surgical steps • - substeps • - tasks • - subtasks • - tool motions • Annotate videotapes and perform analyses on the timing of events. 5. Discussion Hierarchical decomposition can be used to: 1. Evaluate surgeons’ performance 2. Design training for surgery e.g., with augmented or virtual environments Modular sections correspond to our procedural breakdown 3. Evaluate surgeons’ learning 4. Design and evaluate effectiveness of new tools 5. Evaluate different aspects of O.R. layout e.g., monitor display position 6. Preoperative planning of patient-specific surgery 7. Analyze surgeons’ focus of attention at different levels of the hierarchy 8. Improve safety and decrease errors 9. Make a better “fit” between technology and the surgeon. 6. References Cao, C.G.L., MacKenzie, C.L., Ibbotson, J.A., Turner, L.J., Blair, N.P. and Nagy, A.G. (1999). Hierarchical decomposition of laparoscopic procedures. In Westwood, J.D., Hoffman, H.M., Robb, R.A., & Stredney, D. (Eds.), The convergence of physical and informational technologies: Options for a new era in healthcare. (MMVR: 7). Amsterdam: IOS Press, 83-89. Ibbotson, J.A., MacKenzie, C.L., Cao, C.G.L., and Lomax, A.J. (1999). Gaze patterns in laparoscopic surgery. In Westwood, J.D., et al. (Eds.) The convergence of physical and informational technologies: Options for a new era in healthcare. (MMVR: 7). Amsterdam: IOS Press, 154-160. MacKenzie, C.L., Ibbotson, J.A., Cao, C.G.L. and Lomax, A.J. (1998). Intelligent tools for minimally invasive surgery: Safety and error issues. In Proceedings of Enhancing patient safety and reducing errors in health care. Chicago: National Patient Safety Foundation, 226-229. Miller, G.A., Galanter, E., and Pribram, K.H. (1960). Plans and the structure of behavior. New York: Henry Holt and Co. Acknowledgements Thanks to the surgeons, O.R. staff, and patients. Thanks to E. Lee, S. Manske, and B. Zheng. Funded by British Columbia Health Research Foundation (BCHRF) and Institute for Robotics and Intelligent Systems (IRIS), Canada.