Download

1 / 30
300 likes | 308 Views
Screening programme for cancers. CL Teng tengcl@gmail.com. Level of prevention. 1 o. 2 o. Age-specific cancer incidence by ethnicity and sex, West Malaysia 2003. Sex-race specific cancer incidence. GCC Lim, Y Halimah (Eds). Second Report of the National Cancer Registry. Cancer

E N D
Screening programme for cancers CL Teng tengcl@gmail.com
Level of prevention 1o 2o
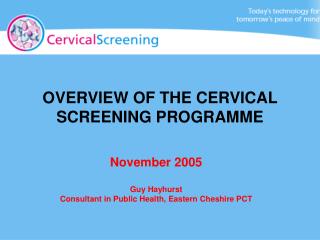
Age-specific cancer incidence by ethnicity and sex, West Malaysia 2003 Sex-race specific cancer incidence GCC Lim, Y Halimah (Eds). Second Report of the National Cancer Registry. Cancer Incidence in Malaysia 2003. National Cancer Registry. Kuala Lumpur 2004. http://www.acrm.org.my/ncr/documents/NCR_2nd_Report/Full_report.pdf
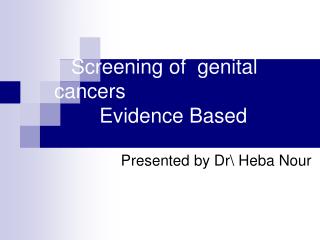
Age-specific cervical cancer incidence by ethnicity and sex, West Malaysia 2003 Race specific cancer incidence GCC Lim, Y Halimah (Eds). Second Report of the National Cancer Registry. Cancer Incidence in Malaysia 2003. National Cancer Registry. Kuala Lumpur 2004. http://www.acrm.org.my/ncr/documents/NCR_2nd_Report/Full_report.pdf
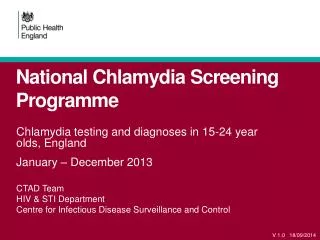
Ten most frequent cancers in males, Peninsular Malaysia 2003
Lung cancer Collapse of the left upper lobe with elevation of the left main bronchus with cutoff of the upper lobe bronchus. Left upper lobe mass at the left hilum. http://www.imagingpathways.health.wa.gov.au/includes/image/nspul_c/XR.JPG
Lung cancer screening Detect mass if >2cm Sputum cytology Five RCTs: CXR sputum cytology 6-monthly vs CXR annually or at the end of 3-year follow-up. Screening detect more lung cancer cases but no difference in survival in the two groups. USPSTF 2004: Do not recommend for or against
Lung cancer screening Low dose Computerised Tomography (LDCT) 13 observational studies (mostly cohort studies [CS). No RCT. LDCT detects 3x more lung cancers than CXR (and smaller cancers). In one study, LDCT detected 23% of nodules (compared to 7% by CXR) but only 3% of the nodules were cancers (low PPV). USPSTF 2004: Do not recommend for or against
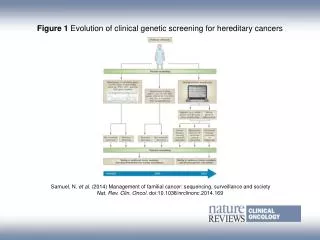
Colon cancer There is a well-described sequence of mutational events that characterize the transition from normal colon epithelium to premalignant adenoma and then invasive adenocarcinoma. http://www.nature.com/nrc/journal/v3/n8/fig_tab/nrc1147_F1.html
Colorectal cancer screening Faecal occult blood test (FOBT) Double contrast barium enema CT colography (virtual colonoscopy) Sigmoidoscopy/colonoscopy
Colorectal cancer screening • Average risk: Age 50 (M&F), FOBT (yearly), flexible sigmoidoscopy (5 yearly), colonoscopy (10 yearly) or barium enema (5 yearly) • High risk: First-degree relative with ca colon. Start screening from age 40 USPSTF, see Ann Intern Med 2002;137:129-31
Incidence of colorectal cancer in Asian vs US and UK populations (1993–97) Sung JJ, et al. Increasing incidence of colorectal cancer in Asia: implications for screening. Lancet Oncol 2005; 6(11):871-876
“Although changes in dietary habits and lifestyle are believed to be the reasons underlying the increase, the interaction between these factors and genetic characteristics of the Asian populations might also have a pivotal role.” Sung JJ, et al. Increasing incidence of colorectal cancer in Asia: implications for screening. Lancet Oncol 2005; 6(11):871-876
Prostate cancer screening • Insufficient evidence to recommend for or against screening for prostate cancer using PSA (prostate-specific antigen) or DRE (digital rectal examination). • PSA detects early-stage cancer but improvement in health outcomes is mixed. • Screening is associated with frequent false-positive result and unnecessary anxiety.
Prostate cancer screening • Current evidence is insufficient to assess the balance of benefits and harms of screening for prostate cancer in men younger than age 75 years (I statement). • Do not screen for prostate cancer in men age 75 years or older (Grade D recommendation) USPSTF, see Ann Intern Med 2008;149(3):185-91
Prostate cancer • USA: most men over the age of 50 years have had a PSA test, despite the absence of evidence from large, randomized trials of a net benefit. Moreover, about 95% of male urologists and 78% of primary care physicians who are 50 years of age or older report that they have had a PSA test themselves, a finding that suggests they are practicing what they preach. http://content.nejm.org/cgi/content/full/360/13/1351
Hepatocellular carcinoma • Inadequate evidence on screening with alpha-fetoprotein and/or ultrasound of the liver for patients with chronic hepatitis B • Only 2 RCTs. • 1. Bi-annual screening with alpha-fetoprotein plus ultrasound vs no screening for five years. More liver cancers were detected in the screened group, but the two groups did not differ significantly regarding liver cancer mortality. • 2. Alpha-fetoprotein plus ultrasound screening vs alpha-fetoprotein screening. This trial, with an inadequate sample size, showed no significant difference between the groups regarding number of cancers detected. http://www.cochrane.org/reviews/en/ab002799.html
Hepatocellular carcinoma • Patients with chronic hepatitis B and C infection especially those who are > 45 years of age, who have concomitant cirrhosis or have a family history of HCC should be examined every 3-6 months with periodic serum alpha-fetoprotein (AFP) measurements and abdominal ultrasound examinations. • Merican I. Screening for hepatocellular carcinoma. Med J Malaysia. 1996;51(1):12-7
Ten most frequent cancers in females, Peninsular Malaysia 2003
Breast cancer screening • Average risk: Age 50-69, 1-2 yearly mammography. • CBE: Do not recommend for or against. • BSE: Do not recommend for or against. Increased risk of false positive results and biopsy. • High risk: Mother/sister had ca breast. Start screening from age 40 USPSTF, see Ann Intern Med 2002;137:344-6
Anderson BO, et al. Breast cancer in limited-resource countries: health care systems and public policy. Breast J 2006; 12 Suppl 1:S54-S69
Modifying factors impacting on cervical neoplasia and persistence of HPV infection ASCUS: atypical squamous cells of undetermined significance Moore MA, Tajima K. Cervical cancer in the Asian Pacific - epidemiology, screening and treatment. Asian Pac J Cancer Prev 2004; 5(4):349-361.
Cervical cancer screening • In Malaysia, all women who are, or who have been sexually active, age 20-65 years, are recommended to undergo Pap smear testing. • If the first two consecutive Pap results are negative, screening every three years is recommended. MOH AMM CPG. Management of cervical cancer. 2003
Pap smear coverage • 1993 to 2003, a total of 3,329,388 pap smears were done • Peak age of the women who had the pap smears: 30-39 years. • Peak age of cervical cancer: 60-69 years. • Pap smear coverage: 0.8 to 2.9%. • Pap smear screening in the country is not strategic. • Nor Hayati O, et al. Malaysian Journal of Medical Sciences. 2006;13(Suppl 1):113.
Screening criteria • Disease. • Sufficient burden of suffering. • Detectable preclinical phase. • Test. • “Sensitive enough”. • “Specific enough” (to reduce FP). • Test, workup and treatment available. • Benefits outweigh harms • Screened cases live longer. • Harms of overtreatment acceptable. • Cost of screening and treatment affordable.
The following statement(s) is/are correct regarding cancer screening tests • False positive is a major concern with many cancer screening tests. • Low-dose computerized tomography detects lung cancer earlier and also prolong life of the screened cases. • Mammography’s benefit is outweighed by its harm in women above fifty years of age. • Alpha-fetoprotein is a good screening test for hepatocellular carcinoma. • Regular colonoscopy is a useful screening test for the detection of colorectal carcinoma. Answer: T, F, F, F, T
The strongest proof that a cancer screening programme is useful is that • Screening detects cancer earlier than usual. • A cheap screening test is available. • Patients are very keen for this screening programme. • Screened cases live longer. • Screening test is non-invasive. Answer: D