Download
1 / 6

E N D
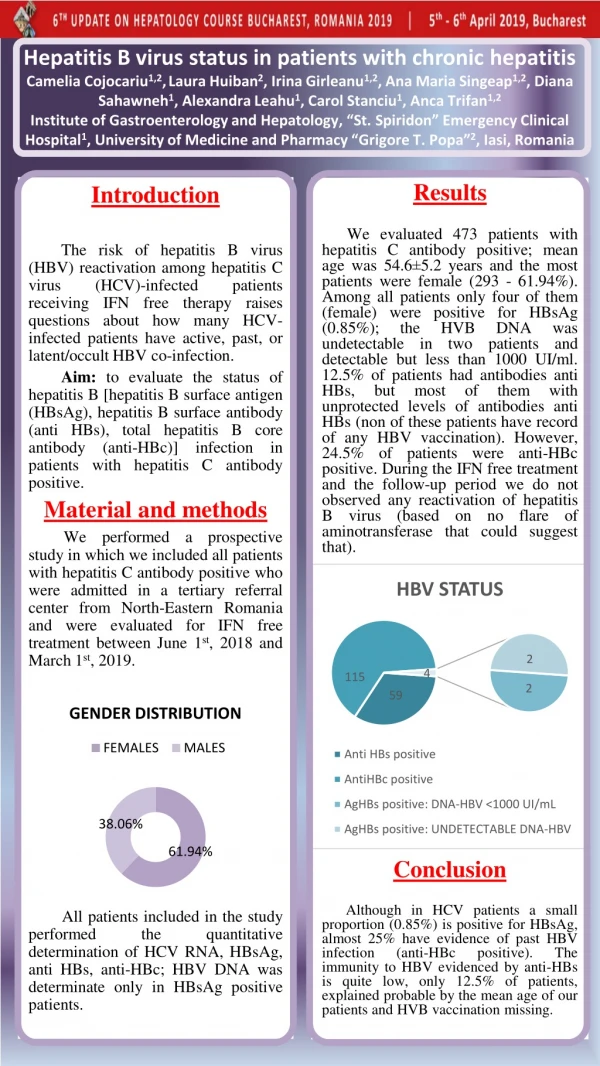
Hepatitis B virus status in patients with chronic hepatitis Camelia Cojocariu1,2,Laura Huiban2, Irina Girleanu1,2, Ana Maria Singeap1,2, Diana Sahawneh1, Alexandra Leahu1, Carol Stanciu1, Anca Trifan1,2Institute of Gastroenterology and Hepatology, “St. Spiridon” Emergency Clinical Hospital1, University of Medicine and Pharmacy “Grigore T. Popa”2, Iasi, Romania Results We evaluated 473 patients with hepatitis C antibody positive; mean age was 54.6±5.2 years and the most patients were female (293 - 61.94%). Among all patients only four of them (female) were positive for HBsAg (0.85%); the HVB DNA was undetectable in two patients and detectable but less than 1000 UI/ml. 12.5% of patients had antibodies anti HBs, but most of them with unprotected levels of antibodies anti HBs (non of these patients have record of any HBV vaccination). However, 24.5% of patients were anti-HBc positive. During the IFN free treatment and the follow-up period we do not observed any reactivation of hepatitis B virus (based on no flare of aminotransferase that could suggest that). Conclusion Although in HCV patients a small proportion (0.85%) is positive for HBsAg, almost 25% have evidence of past HBV infection (anti-HBc positive). The immunity to HBV evidenced by anti-HBs is quite low, only 12.5% of patients, explained probable by the mean age of our patients and HVB vaccination missing. Introduction The risk of hepatitis B virus (HBV) reactivation among hepatitis C virus (HCV)-infected patients receiving IFN free therapy raises questions about how many HCV-infected patients have active, past, or latent/occult HBV co-infection. Aim: to evaluate the status of hepatitis B [hepatitis B surface antigen (HBsAg), hepatitis B surface antibody (anti HBs), total hepatitis B core antibody (anti-HBc)] infection in patients with hepatitis C antibody positive. Material and methods We performed a prospective study in which we included all patients with hepatitis C antibody positive who were admitted in a tertiary referral center from North-Eastern Romania and were evaluated for IFN free treatment between June 1st, 2018 and March 1st, 2019. All patients included in the study performed the quantitative determination of HCV RNA, HBsAg, anti HBs, anti-HBc; HBV DNA was determinate only in HBsAg positive patients.
E-Poster no. 14 Ghioca Mihaela1,4, Iacob Speranta1,4, Ester Carmen1,4, Cerban Razvan1,4, Bardas Alexandru2, Coriu Daniel2,4, Lupescu Ioana3,4, Becheanu Gabriel1, Dobrea Camelia4, Gheorghe Cristian1,4, Gheorghe Liana1,4 1 – Department of Gastroenterology and Hepatology, Fundeni Clinical Institute, Bucharest, Romania 2 – Department of Hematology, Fundeni Clinical Institute, Bucharest, Romania 3 – Department of Radiology, Fundeni Clinical Institute, Bucharest, Romania 4 – “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania Hepatitis C virus (HCV) is known to be a lymphotropic virus, triggering B-cells and promoting B lymphocyte proliferation. It is associated with various lymphoproliferative disorders. Antiviral therapy for HCV, including direct acting antivirals (DAA’s) has proven to be effective in the treatment of HCV-related lymphomas. There are reported only a few cases of lymphoma after viral eradication. De novo occurrence of non-Hodgkin’s lymphoma after SVR with direct acting antivirals for HCV infection Fig. 6 and 7 (2nd patient) – Abdominal MRI revealing a large abdominal adenopathic block and a splenic nodule, suggestive for a tumoral involvement. We report a series of 3 cases with HCV- related liver cirrhosis, two of them with sustained virological response (SVR) after DAA therapy for HCV infection and one with SVR after interferon + Ribavirin therapy, that were diagnosed with large B cell non-Hodgkin’s lymphoma. Fig. 8, 9, 10 – Histopathological and immunohistochemical examination from a abdominal adenopathy biopsy (2nd patient) – Hematoxilin-eosin stain (Fig. 8) with large cell tumoral proliferation, with positive reaction for CD20 (Fig. 9) and Bcl 6 (Fig. 10) The last case is a 67 years-old woman, diagnosed with HCV-related liver cirrhosis in 2007, treated with interferon + Ribavirin in 2006, with SVR, that in August 2018 presented with diffuse abdominal pain and weight loss. The first two cases are those of a 65 years-old woman and a 51 years-old male, diagnosed with HCV-related liver cirrhosis in 2014, respectively in 2017, based on high HVC- RNA level, with compensated disease, that were treated during 12 weeks with Ombitasvir-Paritaprevir/ Ritonavir + Dasabuvir in 2015, and respectively with Ledispasvir + Sofosbuvir in 2017. They obtained SVR after DAA’s and did not present any complications during the follow-up period. The first patient presented 2 years after HCV eradication with large laterocervicaladenopathies and the second one presented in July 2018 with diffuse abdominal pain. Fig. 11, 12, 13 – Thoraco-abdominal CT scan (3rd patient) – showing multiple liver nodules, abdominal adenopathies and costal involvement. Fig. 14, 15 – Histopathological and immunohistochemical examination from a liver biopsy (3rd patient) – Hematoxilin – eosin stain revealing large cell tumoral proliferation. The diagnosis was established trough a close collaboration between the hematologist, radiologist and the anatomopathologist, using imaging techniques (computed tomography scan) and a CT guided lymph node biopsy, respectively liver biopsy were performed and the histopathological diagnosis was large B-cell non-Hodgkin’s lymphoma. Fig.1 and 2. Thoraco-abdominal CT scan (1stpacient) – revealing multiple abdominal adenopathic blocks and thoracic adenopathies. • Direct acting antivirals are the strategy to mainly prevent the occurrence of hepatic manifestations, and also extrahepatic, including lymphoma, but in some rare cases, HCV eradication is not the end point. Fig. 3,4,5 – Histopathological and immunohistochemical examination from a supraclavicular lymphadenopathy biopsy –(1st patient) – Hematoxilin-eosin stain (Fig. 3) with large tumoral cell proliferation, and positive reaction for CD 20 (Fig. 4) and Bcl 6 (Fig. 5)
E-POSTER Nr 17 UPPER GASTROINTESTINAL BLEEDING IN HEPATOCELLULAR CARCINOMA: ROLE OF PORTAL VEIN THROMBOSIS Irina Girleanu, Anca Trifan, Andreea Teodorescu, Camelia Cojocariu, Oana Cristina Petrea, Ana Maria Singeap, Catalin Sfarti, Stefan Chiriac, Laura Huiban, Tudor Cuciureanu, Carol Stanciu “Grigore T. Popa” University of Medicine and Pharmacy, “St. Spiridon” University Hospital, Institute of Gastroenterology and Hepatology, Iași, Romania Introduction Hepatocellular carcinoma (HCC) is one of the most severe complication of liver cirrhosis. The leading causes of death in HCC are hepatic failure and GI bleeding (GIB). Although, variceal bleeding is mostly due to cirrhosis induced portal hypertension (PH), portal vein thrombosis (PVT) induced PH may play a role. HCC is a leading cause of PVT by tumor invasion of the PV. Therefore the aim of this study was to assess the role of PVT development in cirrhotic patients diagnosed with HCC. Material andMethods A prospective analysis was performed on 56 cirrhotic patients diagnosed with HCC who were admitted in a tertiary center from January 2016 to December 2016. After resuscitation, emergency upper GI endoscopy was performed searching for the source of bleeding. Appropriate endoscopic therapy was applied to control bleeding whenever indicated. A full lab and imaging studies were done for all patients. Results Results Out of the 56 cirrhotic patients diagnosed with HCC, 41 patients (73.2%) were males of relatively younger age (mean 53.5 years). HCV was detected in 42.8 % of our HCC patients, while HBV was detected in 19.6 %. All our bleeding HCC patients were cirrhotics with 51 (91.1 %) of them were Child’s class B or C. PVT was diagnosed in 23 patients (41.07%). Out of the 23 patients diagnosed with PVT, 9 patients died during hospitalization and in 18 patientswe failed to control bleeding. Variceal bleeding was the most common cause of upper gatrointestinal bleeding in our HCC patients (96.1 %), while non-variceal sources were detected in only 4 patients (7.1 %). Most of the patients (89.2 %) presented with 1st bleeding episode, while 6 (10.7 %) presented with recurrent bleeding. Conclusions Variceal bleeding is the most common cause of UGIB among HCC patients. PVT plays an important role both in the initiation as well as recurrence of variceal bleeding in HCC patients and negatively influences the patient prognosis.
LIVER INVOLVEMENT AMONG ADULT PATIENTS WITH CELIAC DISEASE Roxana Nemteanu1,2, Alina Plesa1,2, Irina Ciortescu1,2, Irina Girleanu1,2 , Cristina Gorincioi2 , Carol Stanciu2 , AncaTrifan1,2 1. University of Medicine and Pharmacy ”Grigore T. Popa”, Faculty of Medicine, Iasi, Romania 2. “St. Spiridon” Emergency Hospital , Institute of Gastroenterology and Hepatology, Iasi, Romania Introduction: Celiac disease (CD) in multifacedautoimmunedisorderwithseveralextraintestinalmanifestations. The aim of thepresentstudywasto determine theproportion of adult patients CD whohadidiopathichypertransaminasemia at diagnosisandatfollowup, afterinitiation of a gluten freediet (GFD). Materialandmethods: The study included only adult patients with biopsy proven CD evaluated in the Institute of Gastroenterology and Hepatology, a tertiary referral center betweenOctober, 2012- October, 2018, identifiedthroughcomputerizedbiopsyreportsfromtheDepartment of Pathology. Electronic or paperpatientrecordsweresystematicallycollectedand general informationandinformationaboutpresentingsymptoms, serology, laboratoryparameters, andhistologicalassessment of biopsysampleswereobtainedmanuallyandstoredintoone data base. Alanine transaminase (ALT) andaspartatetransaminase (AST) values at diagnosisandafterinitiation of a gluten-freediet (GFD) wereassessed. Results: The studygroupincluded102 patients, 80 (78.4%) females, and the mean age was 40.36±12.31 years (range 20-73years).Whenassessingtheserologicalparameters, IgA-tTGlevels (61.45±76.458 u/mLvs 162.02±106.179 u/mL, P=0.001) correlatedwith intestinal villousatrophy (Marsh 1-2 vsMarsh 3a-c) in CD patients, with a sensitivity of 82.56 % and a specificity of 91.78 %. A total of 48 (47%) hadidiopathichypertransaminasemia at thetime of diagnosis. Of the 48 patientswithhypertransaminasemia at diagnosiswhohadrepeatlaboratory test resultsafterstartingthe GFD, 32(66.6%) normalizedwhereas 16 (33.3%) remainedelevated. Thosewithhypertransaminasemiawereyoungerthanthosewith normal levels (P < 0.0001). Gender, symptoms at diagnosis, and body mass index werenot predictive of elevatedtransaminases. Discussion/Conclusion: Hypertransaminasemiaispresent at diagnosis in a considerableproportion of patientswith CD. Youngerpatients are more likelytohave an elevation in transaminases. Abnormal transaminasesnormalize in themajority of patientsafterinitiationof a GFD.
A total of 22 patients, 16(72.7%) female, mean age 29.78±11.23 years were included. Diagnostic criteria for non‐ceruloplasmin‐bound serum copper, serum ceruloplasmin, 24‐h urinary copper excretion, liver copper content were researched in all patients evaluated, and the presence of Kayser–Fleischer rings and histological signs of chronic liver damage were reached in 12 (54.5%) and 3 (13.6%) of patients, respectively. Patients with neurological symptoms were significantly older at the onset of symptoms than patients with hepatic symptoms (29.1 versus 22.5 years of age, p=0.06), and the neurological symptoms were associated with a significantly longer time from onset to diagnosis than hepatic symptoms (53.4 versus12.8 months, p<0.05). Most patients stabilized or improved on chelation therapy (77.2%), but 18% deteriorated; 2 cases required liver transplant, and 9% died within the observation period. Cirrhosis at diagnosis was the best predictor of death (OR 7.9; 95% CI, 2.9-29.3; P = .023). After initiating treatment, 81% of the patients had a stable or improved course of the disease. Disease progression under treatment was more likely for neuropsychiatric than for hepatic symptoms. WILSON’S DISEASE: CLINICAL PRESENTATION, BIOCHEMICAL PROFILE AND OUTCOME- A 5-YEAR EXPERIENCE OF A TERTIARY REFERRAL CENTRE Roxana Nemteanu1,2, Alina Plesa1,2, Irina Ciortescu1,2, Irina Girleanu1,2 , Carol Stanciu2 , AncaTrifan1,2 1. University of Medicine and Pharmacy ”Grigore T. Popa”, Faculty of Medicine, Iasi, Romania 2.“St. Spiridon” Hospital , Institute of Gastroenterology and Hepatology, Iasi, Romania Introduction Wilson's disease (WD) is a rare genetic disorder related to copper storage, leading to liver cirrhosis and neuropsychological deterioration. Epidemiological and clinical data are limited in the north-eastern part of Romania owing to low disease frequency. Material and Methods: We performed a retrospective five-year analysis (1st January, 2013-31st December, 2018) of medical records of all adult patients diagnosed with WD, examined at the Institute of Gastroenterology and Hepatology, Iasi, Romania. Clinical manifestations, biochemical, and histological profiles were assessed for each patient to determine presentation, diagnostic course and long‐term outcome. Results A total of 22 patients, 16(72.7%) female, mean age 29.78±11.23 years were included. Diagnostic criteria for non‐ceruloplasmin‐bound serum copper, serum ceruloplasmin, 24‐h urinary copper excretion, liver copper content were researched in all patients evaluated, and the presence of Kayser–Fleischer rings and histological signs of chronic liver damage were reached in 12 (54.5%) and 3 (13.6%) of patients, respectively. Patients with neurological symptoms were significantly older at the onset of symptoms than patients with hepatic symptoms (29.1 versus 22.5 years of age, p=0.06), and the neurological symptoms were associated with a significantly longer time from onset to diagnosis than hepatic symptoms (53.4 versus12.8 months, p<0.05). Most patients stabilized or improved on chelation therapy (77.2%), but 18% deteriorated; 2 cases required liver transplant, and 9% died within the observation period. Cirrhosis at diagnosis was the best predictor of death (OR 7.9; 95% CI, 2.9-29.3; P = .023). After initiating treatment, 81% of the patients had a stable or improved course of the disease. Disease progression under treatment was more likely for neuropsychiatric than for hepatic symptoms. Conclusions: WD patients had an overall good long-term prognosis. Early diagnosis, at a precirrhotic stage, might increase survival times and reduce the need for a liver transplant.





