Download
1 / 52
520 likes | 767 Views
Additional Verbal Communication & Reflective Listening Tools: . Questioning: asking open, closed or leading questions to gain information, encourage the speaker to tell her story, and gain clarification.

E N D
Additional Verbal Communication & Reflective Listening Tools: Questioning: asking open, closed or leading questions to gain information, encourage the speaker to tell her story, and gain clarification. Funneling: use of questions to guide the conversation from a broader area to more specific area. Paraphrasing: a brief, succinct statement reflecting the content of the speaker’s message. Reflecting Feeling/ Selective reflection: a statement, in a way that conveys understanding, of the feeling that the listener has heard. Empathy Building: Make the listener understand that his/her feelings have been well understood. Summarizing: a statement of the main ideas and feelings to show understanding.
Barriers to Effective Communication: A barrier to communication is something that keeps meanings from meeting. Meaning barriers exist between all people, making communication much more difficult than most people seem to realize. It is false to assume that if one can talk he can communicate. Because so much of our education misleads people into thinking that communication is easier than it is, they become discouraged and give up when they run into difficulty. Because they do not understand the nature of the problem, they do not know what to do. The wonder is not that communicating is as difficult as it is, but that it occurs as much as it does." - Reuel Howe, theologian andeducator
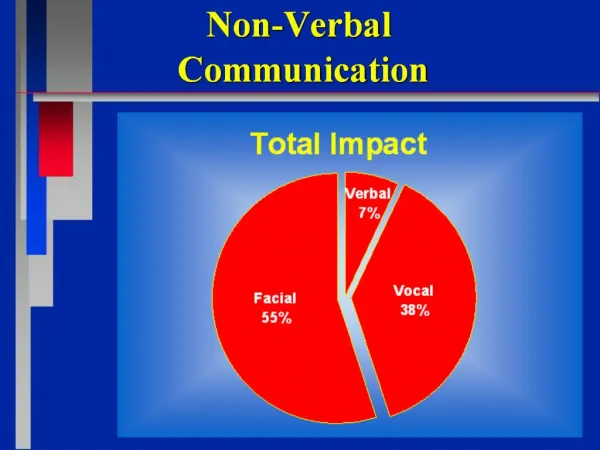
Barriers to Effective Communication: • Verbal Communication Barriers:Like Shouting, Ordering, Criticizing, Demoralizing, Threatening, Advising, Directing, Blaming, Preaching, & Refusing to speak. • Nonverbal Communication Barriers: Like Flashing or rolling eyes, Quick or slow movements, Arms crossed, legs crossed, Gestures made with exasperation, Slouching, hunching over, Poor personal care, Doodling, Staring at people , Avoiding eye contact, & Excessive fidgeting with materials.
SO Effective Communication . . • is two way. • involves active listening. • utilizes feedback. • is free of stress. • is clear. • reflects the accountability of • speaker and listener.
PSYCHOTHERAPY/ COUNSELLING: • Counseling and psychotherapy are both ‘talking therapies’ that offer people a chance to change how they feel and to live better. • A counselor or therapist isn’t there to give you advice or to tell you what to do, but will listen to you carefully and engage you in a conversation that can help to clarify aspects of your life that may be causing you distress or confusion.
Psychotherapy takes place in the context of a solid, trustworthy working relationship between the client and the therapist. It helps create the context, the insight, the vision, the under standing, and the support within which durable growth and desirable change can take place. Psychotherapy is not advice giving, but it can involve giving advice. It empowers the client to come to useful personal understanding, to make clearer choices, and to a more achieve lasting independence.
Psychotherapy is a process of discovery - - a learning and an unfolding process. • Psychotherapy assumesthat there are aspects of our lives of which we are not fully aware. • Our thoughts, feelings, behaviors, dreams, and our reactions to people and events are based on hidden assumptions, expectations, and on memories of earlier events. • Our lack of awareness, lack of skill and choice, and many of our old wounds limit much of our untapped creative energy. • Psychotherapy affords an opportunity to uncover, describe, explore, learn about, and appreciate our perceptions, our hidden assumptions, the ways we have adapted to life -- as well as how all these have evolved.
The aims of counselling: • Everyone has different ways of coping with their personal difficulties. People often deal with stressful situations and events by talking to their partner, a family member or a friend. However, in certain situations, talking to a professional counsellor may be more helpful. • Counselling can help people to: • discuss their problems honestly and openly, • deal with issues that are preventing them from achieving their goals and ambitions, and • have a more positive outlook on life.
Admitting you need help is a positive step!!!!! • At some stage, you will probably experience feelings of stress, disappointment and grief. At these times, seeking assistance can help you deal with your feelings and emotions. • Counselling can be a positive way of addressing any unresolved issues that you have. It can help you to understand your problems better, rather than ignoring them and hoping that they will go away, only for them to come back later. It can also give you a better understanding of other people's points of view.
Attributes of Counselling: • Unconditional Positive Regard: (Non-judgmental, deep, trusting and positive feelings for the patient). • Empathic Understanding: (Accurately perceive and understand patient’s feeling). • Warmth and Geniunity: (Spontaneous, open, non-defensive, respectful and tactful towards patient). • Clarity: (Clear, Explicit and ensure a successful communication). • Here and Now: (successfully handle the distress of the past not to effect the present and focus more on present day issues).
What To Expect: • Relationship of mutual trust and caring. • Provision of Reassurance. • Provision of Clarification and Explanation. • Freedom of expressing feeling and emotions. • Achievement of deeper and clearer understanding of issues . • Identification of various choices and options. • Training of Decision making skills. • Training of Problem Solving skills. • Training of necessary Coping skills. • Support without challenging.
Myths about therapy: • I don't need a therapist. I can just talk to my friends. Therapists are professionally trained as listeners to help you get to the root of your problems and guide you to a solution. • Therapy is only for mentally ill people who can't handle their problems. Therapy helps you learn tools and techniques to improve your intimate relationships and quality of life. • The therapist will fix my problems.The therapist focuses on the unhealthy patterns and symptoms in your life that you need to change.
A Case Scenario: A young couple relocates to a new area. They are hundreds of miles away from family and friends. The husband works full time and the wife is a stay at home mom. They have been in their new area about 1 year. The wife is becoming bored, lonely and depressed as she does not have any friends or significant social life. Her husband talks a lot about work when he comes home. He then spends an inordinate amount of time talking on the phone with his work colleagues and friends that he has made. He goes out frequently without his wife often staying out through the wee hours of the morning. Is this a case where marriage counseling is needed?
A gut reaction would be to answer this question as yes, absolutely. There are some serious and significant issues developing in this relationship. A professional counselor should be able to identify the root of the problems that both individuals in this relationship are not seeing or have ignored. Once these problems have been diagnosed then the counselor can establish a workable plan that will allow this couple to resolve these major issues.
In looking a little deeper at this situation marriage counseling may not be needed right away. Why would I say that? Well, we don't know if this couple has ever even discussed this situation or the problems that the wife is perceiving. Hard to imagine but the husband may not even be aware that there is a problem. If the wife never speaks up to express her feelings he may think everything is fine, so why change.
The first thing that needs to occur here is the wife needs to communicate to her husband how she feels and make him aware of these issues. I know, it's hard to believe that he doesn't see it but some people are just that oblivious or just don't care OR she is putting up a good front and doesn't show that anything is wrong.
Another deeper issue in this situation is why doesn't this wife have any friends or why isn't she developing a social network of her own? Has she made any attempt or effort to meet people and make friends? If she is a stay at home mom with young kids then certainly there are play groups, play dates, support groups, child activity centers, and community events centered around children that she could become involved in in order to meet other like moms that may be in her situation.
Yes, the husband has issues in this relationship but the wife is relying solely on him for support. She needs to make an effort to take care of herself.
2D &3D images of Sun
INFORMATIONAL CARE: • It is Provision of information to patients regarding the treating physician (Doctor), the illness (Disease) and the treatment (Drugs).
BACKGROUND: • The community recognizes that patients are entitled to make their own decisions. • In order to do so, they must have enough information about their condition, investigation options, treatment options, benefits, possible adverse effects of investigations or treatment, and the likely result if treatment is not undertaken. • It is not possible however, to provide complete information or to predict outcomes or assess risks with certainty, and patients need to be aware of this uncertainty.
The Amount Of Information: • The amount of information provided, timing, setting, language, along with inclusion of family and support, and exclusion of distraction – need to be tailored according to individual needs of the patient, the stage of illness and most importantly patient’s knowledge, understanding and expectations about his/her illness and its management.
The Quality Of Information: • Once you have a clearer understanding of what information your patients and their carers want, the next step is to identify appropriate information resources. • In addition to assessing information as health professionals, patients and their families increasingly want to be proactive and seek information for themselves.
The benefits of providing information to patients: • There is growing recognition within the HealthCare Systems, of the value of providing patients with information about their illness and possible treatment options, particularly in response to concerns about quality assurance and consumer satisfaction. • Moreover, there is evidence that the provision of such information can reduce levels of anxiety and depression and significantly affect the course of recovery, facilitating faster convalescence and potentially reducing length of hospital stay, improve medication compliance, and follow ups.
INFORMATION TO BE GIVEN: • The possible or likely nature of the illness or disease; • The proposed approach to investigation, diagnosis and treatment; • Other options for investigation, diagnosis and treatment; • The degree of uncertainty of any diagnosis arrived at; • The degree of uncertainty about the therapeutic outcome; • The likely consequences of not choosing the proposed diagnostic procedure or treatment; • The time involved; and the costs involved.
PRESENTING INFORMATION: • The way the doctor gives information should help a patient understand the illness, management options, and the reasons for any intervention. • It may sometimes be helpful to convey information in more than one session. • Information should be provided in a form and manner which help patients understand the problem and treatment options available, and which are appropriate to the patient’s circumstances, personality, expectations, fears, beliefs, values and cultural background.
The doctor should: • Communicate information in a form the patient should be able to understand; • Repeat key information to help the patient understand and remember it; based on his/her knowledge, understanding, and expectations. • Give written information or use diagrams, where appropriate, in addition to talking to the patient; • Pay careful attention to the patient’s responses to help identify what has or has not been understood; • The patient should be encouraged to reflect on opinions, ask more questions, consult with the family, a friend or advisor.
Patient information should be: • • Clear and understandable • • Delivered in everyday language • • Accessible • • Evidence based (where appropriate) • • Sensitive to gender, age, cultural needs • • Cost-effective • • Up to date • • Relevant to the patient’s stage in the care pathway
WITHHOLDING INFORMATION: • Information should be withheld in very limited circumstances only: • If the doctor judges on reasonable grounds that the patient’s physical or mental health might be seriously harmed by the information; or • If the patient expressly directs the doctor to make the decisions, and does not want the offered information. Even in this case, the doctor should give the patient basic information about the illness and the proposed intervention.
Thinking point: “Information is a source of learning. But unless it is organized, processed, and available to the right people in a format for decision making, it is a burden, not a benefit.”
Case Scenario # 1 • You are a 25-year-old female medical student doing a rotation in an HIV clinic. Sara is a 30-year-old woman with advanced HIV who dropped out of college after she found that she contracted HIV from her husband, who has hemophilia. In talking to Sara, it turns out you share a number of things--you are from the same part of Lahore originally, also have young children, and like to cook. Later in the visit, when you suggest that she will need some blood tests, she gets very angry and says, "What would you know about this?" • What happened? And how will you calm her down?
Case Scenario # 2 • Ayesha is originally from Islamabad. For the past month, however, you've been noticing that she has missed classes and teachers have been mad at her because she is not following through on her studies and other responsibilities. You happened to find out that she has been sad, crying frequently, and taking naps during the day. She refuses her friends' invitations to go out, saying she’d rather be alone to study, but she just sleeps. When she is around others, such as her roommate, she started to make self-depreciating remarks about herself, and doesn't accept people's reassurances. She has started to make real weird jokes about death, to which people don't know how to respond.
WHAT TO DO? WHAT HAPPENED? • Her roommate, Hira comes to you and says she is concerned about Ayesha, because tonight A said she was going to spend the night in a hotel to "get away from everyone.” • Questions: • What symptoms of depression Ayesha has indicated? • What would you say to Hira (the roommate)? • What is your role here? • What might you do to help in this situation? • If you are able to talk to Ayesha, what would you ask/say? What campus resources would you suggest for her?
CRISIS: • Crisis is a crucial stage or turning point in the course of one’s life. • It is a situation of extreme danger, instability, discomfort, difficulty, disorganization, disequilibrium , and disaster. • However, it holds a potential for great personal growth, requiring a deep and insightful decision – making which may lead to a permanent change in one’s life. • Resolution may result in increase or decrease or return to baseline of individual’s level of functioning.
Crisis: (A definition according to Ministry Of Health, Ontario) • An emotional upset, arising from situational, developmental, biological, psychological, socio-cultural, and/or spiritual factors. • This state of emotional distress results in a temporary inability to cope by means of one's usual resources and coping mechanisms. • Unless the stressors that precipitated the crisis are alleviated and/or the coping mechanisms are bolstered, major disorganization may result. • It is recognized that a crisis state is subjective and as such may be defined by the client, the family or other members of the community.