Download
1 / 20
210 likes | 503 Views
Fever in Children. Year 1 Derby VTS Teaching. Aims and Objectives. What is fever? Using 4 case studies we will consider: How to differentiate between children with and without serious illness when there is no obvious cause in particular focusing on the history and examination

E N D
Fever in Children Year 1 Derby VTS Teaching
Aims and Objectives • What is fever? Using 4 case studies we will consider: • How to differentiate between children with and without serious illness when there is no obvious cause in particular focusing on the history and examination • If and how an elevated temperature should be managed including strategies to manage parent’s fears.
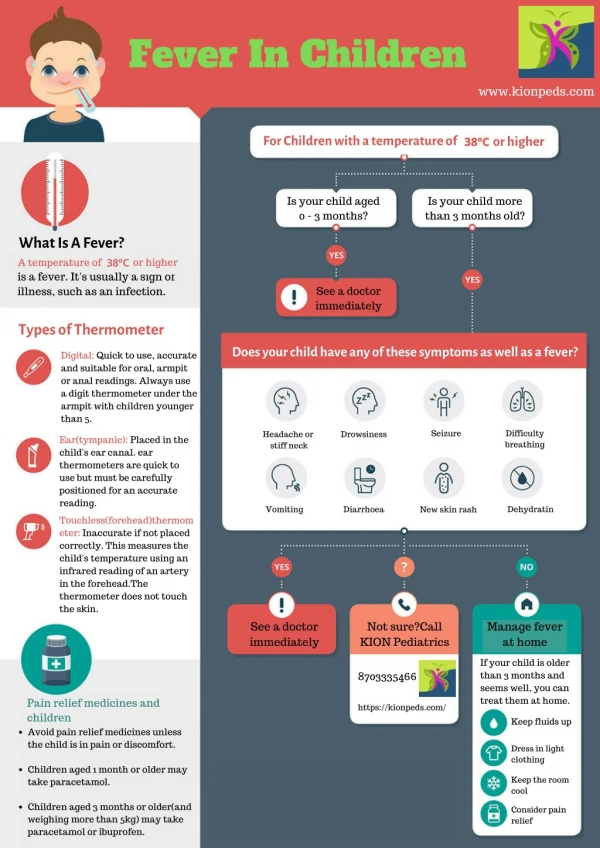
Fever (1) • Defined as1: • Rectal temperature above 38c • Oral temperature above 37.8c • Axillary temperature above 37.2c • Tympanic temperature above 37.8 • In 2-6 year old children diurnal variation of +/- 0.9c • Important physiological response during illness.
Fever (2) • A viral or bacterial infection can reset the thermoregulation centre in the hypothalamus producing an elevated temperature1. • Most cases of fever are due to benign viral illnesses, unfortunately serious infections such as meningitis and pneumonia may initially present with fever and the challenge is to identify those developing a serious infection1. • The most common bacterial infection in febrile children is a urinary tract infection1.
Cases • Divide into 4 groups (Cases 1-4) • Discuss the case and answer the questions (15 minutes) • Nominate two members of the group to present the case and your group’s answers.
Case 1 • How to measure temperature? • NICE Guidelines
“Treating” fever • Most children are not uncomfortable until fever reaches 39.5-40C1 • May consider not treating the fever1 • Paracetamol and ibuprofen may be used1 • Calculate the dose required carefully and ensure parents know how to measure that dose. 1
Fever Phobia • Studies have shown that a high percentage of parents feel fever can have serious consequences. 1 • It is underlying illness rather than fever itself which is responsible for most morbidity. 1
Vaccination • Before introduction of Hib and pneumococcal conjugate vaccines, the reported incidence of serious bacterial illness in a child with a fever who is <36 months ranged from 3-13%. 1 • Since these vaccines were introduced liklihood of serious bacterial infection in children with a fever 3-36 months decreased to less than 2%.1 • Recent vaccination may be an aetiological factor for fever- can be expected 12-24hrs post DPT vaccination and can last 24-48hrs. 1
Case 2 • Increased risk of serious bacterial infection because she has a significant temperature for her age and she is only 6 weeks old. 1 • Referral to secondary care would be appropriate. • Introduction to traffic lights handouts (NICE guidelines)
When to admit to hospital? • Any RED features Admit • Amber features Use clinical judgement but it may be appropriate to monitor the situation in the community • Only Green features Usually safe for management at home
Case 3 • How does your practice triage telephone calls from parents who phone about a child with a fever? • Often a face to face clinical assessment will be necessary to make a safe clinical judgement about fever in young children so some practices have a policy of seeing all under 5’s in the emergency surgery.
Case 3 • Moderate risk category • Liklihood of bacteraemia is low as Ryan is up to date with immunisations • May have an occult pneumonia • UTI is uncommon in a boy of this age who has no symptoms1
Case 4 • Judging a temperature by touch is unreliable • Oral or tympanic temperature is indicated in a child of David’s age • How might you differentiate between isolated delirium and a globally impaired CNS function?
Delirium • Uncommon symptom in children1 • Fever alone is a common reason when it does occur1 • Usually quick recovery (minutes to hours) 1 • Normal neurological examination1 • Warning: Delirious behaviour can also be a symptom of acute encephalopathy1
Take Home Points • The younger the age, the greater the risk of a serious bacterial infection underlying the fever • Use NICE traffic light system to guide management References • 1.Fever in Children, Scotland PBSG Learning Programme. Accessed at www.nes.scot.nhs.uk/medicine/gpcpd/pbsg/ • 2.NICE guideline 47. Feverish Illness in Children: Assessment and initial management of children younger than 5 years.