Download
1 / 28
300 likes | 775 Views
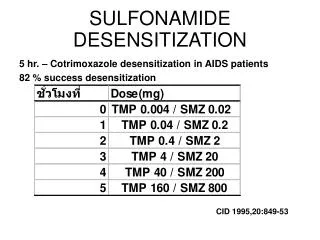
Aspirin Exacerbated Respiratory Disease Diagnosis and Desensitization. Sandra C Christiansen MD Kaiser Permanente & UCSD. Aspirin/NSAID Sensitivity. Pseudoallergic reactions: urticaria/angioedema Respiratory, including naso-ocular and/or asthma

E N D
Aspirin Exacerbated Respiratory DiseaseDiagnosis and Desensitization Sandra C Christiansen MD Kaiser Permanente & UCSD
Aspirin/NSAID Sensitivity • Pseudoallergic reactions: • urticaria/angioedema • Respiratory, including naso-ocular and/or asthma • Rarely: anaphylactoid reaction with laryngeal or GI sx • Prevalence: • 0.2% general population • 8-19% asthmatics • 30-40% polyps & sinusitis • AERD (ASA quatrad): • asthma, sinusitis, ASA sensitivity, nasal polyps
Clinical AERD presentation (1) • Sequence of symptoms • Rhinitis at an average age of 30 years, related to a flu-like infection in half of patients; possibility of ETS or diesel particulate exposure • Asthma (2 years later) • Aspirin intolerance and nasal polyposis (4 years later) with anosmia or hyposmia • Women • Outnumber men by 2.3:1 • More progressive and severe • Atopy – one third to two thirds Szczeklik et al Eur Respir J 2000
Clinical AERD presentation (2) • Most patients with AERD have moderate or severe persistent asthma. • Inhaled corticosteroids; 80% • Oral steroids; 51% Szczeklik et al Eur Respir J 2000
Clinical AERD presentation (3) • After ingestion – acute asthma attack occurs within 3 hours, usually accompanied by profuse rhinorrhea, conjunctival injection, periorbital edema, and sometimes a scarlet flushing of head and neck Szczeklik et al J Allergy Clin Immunol 1999 • AERD is a common precipitant of life-threatening attack of asthma (7 out of 92 asthmatics who underwent mechanical ventilation) Picado et al Eur Respir J 1989 • 25% of asthmatic patients requiring emergency mechanical ventilation – AERD (147 asthmatics) Marquette et al Am Rev Respir Dis 1992
Prevalence of AERD according to severity of bronchial hyperresponsiveness P < .01
Prevalence of AERD according to sputum eosinophil count P < .05
Aspirin Sensitivity Correlates with Potency of COX-1 Inhibition
Cyclooxygenase pathway • COX-1 and COX-2 have molecular weights of 71 kd and 60% homology • COX-1 constitutive form • COX-2 induced during inflammation and enhances synthesis of inflammatory prostanoids
PGE2 • Reduce LT biosynthesis through inhibition of 5-LO • Inhibits cholinergic transmission • Prevents discharge of granular mediators from mast cells • Prevents ASA-precipitated bronchoconstriction and the expected rise in urinary LTE4
PGE2 administration by inhalation inhibits aspirin induced bronchoconstriction Sestini et al AJRCCM 1996 • Selective COX-2 inhibitor(celecoxib, rofecoxib) – preserve PGE2 and do not cross-react with ASA Stevenson et al J Allergy Clin Immunol 2001 Szczeklik et al Clin Exp Allergy 2001
Fig. 3. Counts of cells immunostaining for 5-LO pathway enzymes in bronchial mucosal biopsies from patients with AIA (n = 10), withATA (n = 10), and N subjects (n = 9), taken 20 min after bronchoscopicchallenge with placebo solution. Enzymes are 5-LO, FLAP, LTA4hydrolase (LTA4H), and LTC4 synthase (LTC4S). Horizontal bars,mean±SEM. All significant comparisons between subject groups (P< 0.05 Mann-Whitney) are indicated. Cowburn et al J Clin Invest 1998
What are likely effects of ASA desensitization treatment ? • Early decongestion nasal tissues: (1) Inhibits COX-1 and 2 : stops synthesis of PGD2 (2) Blocks or decreases LT1&2 receptors on capillaries (3) Blocks mast cells from releasing more histamine Early effects bronchial: down regulates cysLT1R Later anti-inflammatory effects of ASA: (1) Inhibits cellular transcription in ? which or all cells (2) Inhibits expression of cys LT1 receptor ? cysLT2R (3) Activates apoptosis of eosinophils ? mechanism (4) Stops discharge MBP and ECP from eosinophils
Polyp sinus surgery before and after ASA desensitization • AERD patients average one sinus/ polyp operation every 3 years: • After ASA desensitization: • Average revision operation: one every 10 years • Majority stopped or slowed growth of polyps • With decrease in polyps, decrease infections • Decrease in need for prednisone bursts
‘How We Do It’Preparation for ASA Challenge • Consult for AERD • 2 week prechallenge nursing checklist, review medications (singulair, prednisone dose, frequency of SABA) • Advise MD if changes required • Hold antihistamine 48 hours prior, SABA after midnight pre challenge
Toradol Challenge • Nasacort spray vial soln 8mg Toradol/cc • Monitor spirometry, symptom scores, VAS, PIF • IV, one on one nursing • Dosing 30”intervals, NS, 1spray (1.04mg) to 6 sprays each nostril (12.48mg)
ASA Challenge/Desensitization • FEV1 >70% • Monitor spirometry, symptom scores, VAS,PIF • IV, one on one nursing • Dosing 3’ intervals, usual mg 20.25, 40.5, 81, 162.5, 325, 650 • Maintenance 650 bid for 6-12 months then 325 bid
Risk Factors for Severe Reaction • Drop in FEV1>30% • Lack of LT modifier • Baseline FEV1 <80% • Prior asthma related ED visit • 75% threshold dose 45 or 60mg • 3% initial reactions 150-325, no reactions at 650 for threshold dose A. Hope et al JACI 2009; 123:406-10
ASA Reaction Treatment • Ocular, topical antihistamine • Nasal antihistamine, topical decongestant • Laryngeal, racemic epinephrine (2.5mg/2cc) • Bronchial, Nebulized Albuterol • GI, IV Ranitidine • Urticarial, IV Benadryl 50mg • Shock, Epinephrine IM Epipen
Long Term AERD Tx Outcomes • 1995-2000 Scripps Clinic GCRC, 172 enrolled, written and telephone f/u • 14% dropout, 78% of remaining 148 improved, 87% for 110 with >1 year f/u • Onset of improvement 6mo,# sinus infections, prednisone bursts, smell score, nasal-sinus and asthma symptoms • 1-5 year ED, Hospitalization, ESS p<.0001 M Pilar Berges-Gimeno et al JACI 2003;111:180-6
Economics of ASA Treatment for AERD • Ambulatory desensitization for AERD cost $6768 per quality-adjusted life year (QALY) • Saved $18.54 per additional symptom-free day • Remained cost effective across a wide range of assumptions (<$50,000 per QALY saved) M. Shaker et al JACI 2008;121:81-7