Download
1 / 52
550 likes | 953 Views
Duchenne Muscular Dystrophy. By Steven Shikhel . Guillaume-Benjamin-Amand Duchenne. Duchenne Muscular Dystrophy (DMD). Guillaume-Benjamin- Amand Duchenne credited with discovery dystrophy voluntary muscles progressively weaken Effect starts and is worse at extremities, mostly legs

E N D
Duchenne Muscular Dystrophy By Steven Shikhel Guillaume-Benjamin-Amand Duchenne
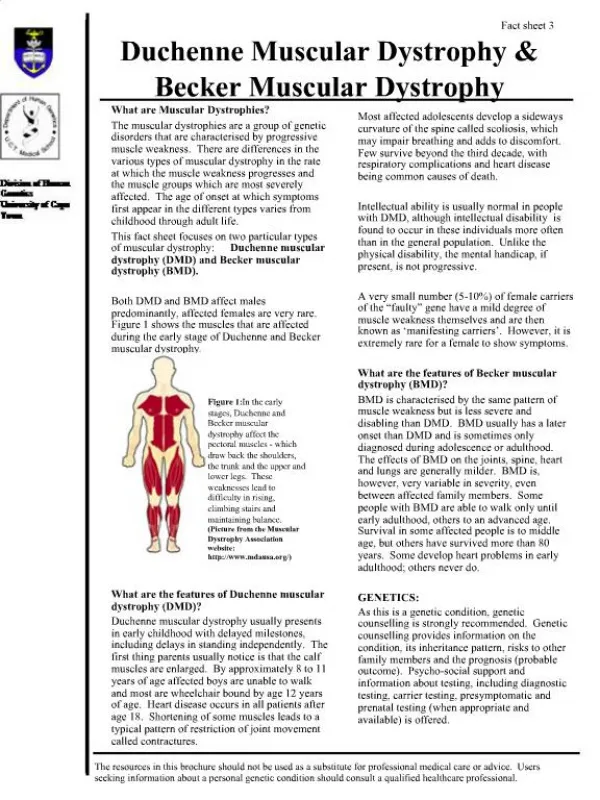
Duchenne Muscular Dystrophy (DMD) • Guillaume-Benjamin-Amand Duchenne credited with discovery • dystrophy • voluntary muscles progressively weaken • Effect starts and is worse at extremities, mostly legs • Timeline • 2-3 years start seeing reduced motor function • 6-11 steady decline in strength • 9-13 failure to walk • 15-25 death most common
Genetics • Most common X-chromosome linked genetic disorder • Xp21- dystrophin gene • approx 1 in every 3500 males are infected • recessive • Allelic with Becker Muscular Dystrophy • Result of absence or mutation in protein Dystrophin
Genetics • Mutations in gene Xp21 cause a lack of dystropin and leads to sarcolemmal instability and disruption of the dystrophin-associated protein complex (DAPC) • Microdisruptions in sarcolemmaleads to increase levels of Ca2+ and alterations in Ca2+ mediated signaling and calpain-mediated proteolysis-protein degredation • Signaling molecules, neuronal nitric oxide synthase (nNOS), Grb2 and calmodulin, are disrupted and cause repetitive cycles of degeneration followed by muscle regeneration
Treatments • Corticosteroids- minimal short-term benefits; prednisone+deflazacort • Gene-based therapies- viral vectors are used to deliver functional dystrophin to muscle fibers or correct dystrophin mutations using exon-skipping strategies • Cell-based therapies- use transplantation of various precursor cells like ex-vivo manipulation muscle side population cells into muscle fibers • Pharmaceutical strategies- aminoglycoiside antibiotics- enable read-through of mutant stop codons in the gene encoding dystrophin, thus enabling full-length dystrophin to be translated • Problem with all these therapeutics is achieving wide distribution to all skeletal muscle
Treatments to decrease downstream effects • Reverse muscle degeneration and increase calpain-mediated proteolysis • Increase endogenous levels of utrophin at the sarcolemma of dystrophin skeletal muscle fibers (will be discussed more later) • Myostatin a negative regulator of muscle growth and beta2-adrenergic receptor agonist albuterol to increase calpain activity (will be discussed more later)
Objective • I will be examining at the molecular structures of Dystrophin, Utrophin, and Myostatin to better understand Duchenne Muscular Dystrophy and possible therapeutics
Dystrophin • Thought to function structurally but precise function remains unknown • Part of spectrinsuperfamily-Closely related protein members that bind to actin and contain differing numbers of tandem homologous repeats comprised of a three-helix motif • Spectrin • Alpha-actinin • Dystrophin • Utrophin • fimbrin • Full Length dystrophin • 3685 amino acids • Molecular mass of 427 kDa
Dystrophin Domains • domains • 30 kDa N-terminal Domain* • Central domain which compromises 24 spectrin-like three-helix bindle motifs • C-terminal region which interacts with tansmembrane proteins beta-dystroglycan and indirectly with dystrophin-glycoprotein complexes • WW, EF, ZZ motifs *disease causing mutations of N-terminal region because of deleterious affect through regions binding to F-actin
Cell Biology of Dystrophin • Located on sarcolemma- muscle membrane • Binds to intracellular cytoskeleton by associating with actin filaments on N-terminus and binds to β-dystroglycan on C-terminus • Binds to extracellular α-dystroglycan which binds to β-dystroglycan, which acts as a receptor to protein laminin • Link between extracellular matrix and intracellular actin cytoskeleton • Provides structural stabilization
mdx Mouse • Duchenne Mouse model- absence of dystrophin • Point mutation putting a stop codon into exon in gene coding of dystrophin • Most interesting is the multi-stages seen • Postnatal muscles appear histologically normal • 3-4 weeks acute phase of necrosis • Muscle recovery after approx 30-40 days old • Reports of occasional regneration in 120-270 days old • Stabilization associated with hypertrophy of the limb muscles and with some evidence of degeneration • However accumulation of Ca2+ and creatinekinase is elevated • 15 months atrophy evident and progressing • Most likely due to changes in signaling molecuels
Proposed Function of Dystrophin • Mechanical damage hypothesis- dystrophin provides mechanical stability to muscle plasma membrane against stresses placed on during normal contraction • Leaky membrane theory- muscle damaged due to faulty protein on membrane causing instability and permeability with chronic myofiber leakage • Calcium Theory- prevents loss of calcium homeostasis which possibly results from abnormalities in specific and novel ion channels in dystrophin tissue
Structure of N-terminal Actin Binding Domain (ABD) • Antiparallel dimer of two ABD each compromising two calponin homolgy domain CH1 and CH2 linked by a central helix • Sequence from which ABDs are proposed to derive is homologous to smooth muscle protein calponin hence calponin homology domain • Spectrin Superfamily
CH2 –formed from a scaffold of seven helices • Major helices A, C, E and G –core CH2 • Helices B, D and F are short two and three turn helices that connect the major structural elements • C, E, and G approx parallel and form triple helical bundle • Ch1 and CH2 linked by alpha helix I • I Dystrophin Monomer • A helix roughly perpendicular CH1 • B and D helices not present in CH1 domain are are replaced with loop regions and an extra turn at N-terminal end of E helix • Ch1 and CH2 alpha helical globular folds
Dimer contact by extensive contacts between helix I and corresponding region in other monomer and interaction with C termini • Hydrophobic patches formed by Val-123, Met-124, Ile-127, Met-128, Ala-129, Gly-130, and Lue 131 on face of helix I and Val-243 and Ile-245 on C terminus are buried upon dimer formation
Dystrophin Dimer • Val123 • Met124 • Ile127 • Met128 • Ala129 • Gly130 • Leu131 • Val243 • Ile245 • 19% of total surface area monomer is excluded from solvent • Shape complementarity and total area of interface imply stable dimer Yellow-hydrophobic patches
Structural basis for Phenotypes • 2/3s of muations are from large deletions and duplications in genes • 1/3 from small deletions and missensemutations, some found in ABD • Details on one DMD patient with a Leu-54 → Argmutation, abnormal • Produces 20% of normal dystrophin • Most DMD patients produce little or none • Proteins are normal sized and correctly localized at sarcolemma • Phenotype is still severe • Located on hydrophobic face CH1 domain C helix where its leucinesidechain and conjunction with leucine 50, 51, 53 and 57 contribute to core of domain • Region of C helix packs against Ala80. Val 83 and Leu84 on hydrophbc surface of helix E, • Ile114, and Trp118 from helix G • The substitution Arg 54-Leu would be expected to destabilize the domain fold by introduction of large charged sidechain into this hydrophobic environment • Pathogenic in-frame deletions of exons 3 and 5 of dystrophin gene have been characterized • Deletions in exon 3cause variable phenotypes • Deletions in exon 5 cause patients with reduced levels of dystrophin
DMD patient with Leu54-Arg mutation CH1 domain DMD patient Ala80 Leu 50,51,53, 57 Val83 Leu84 Trp118 Ile114 a
Mechanism of Actin-Binding • Three actin binding sites (ABS) have been proposed for residues in dystrophin ABD involved to binding of F-actin • NMR studies suggest two regions ABS1 residues 17-26 and ABS3 residues 131-148 might be involved in binding to actin residues 83-117 and 350-375 respectively • ABS1 and ABS3 are located on helix A of CH1 and CH2 respectively • ABS2 located on E and F helices of CH1 • Three ABSs don’t form surface together that could bind dystrophin onto actin • Suggests that a conformational change bringing ABSs regions closer to form a binding surface • Within ABD, CH1 appears to form major contacts with actin because CH1 domain alone is able to bind whereas CH2 domain cannot • CH2 does contribute because binding affinity is greater in complete ABD than in isolated CH1
ABS1 17-26 ABS2 88-116 ABS3 131-148 ABS11 ABS2 Dystrophin Actin BindingSites ABS33
Dystrophin Structure Conclusion • Different missense mutations have been found including Leu54→Arg*, Ala169→Asp, Ala171 →Pro, and Tyr231 →Asn all on hydrophobic core but none lie within ABS1-3 • Internal location of residues implies that mutations alter protein function by destabilization of the domain fold as opposed to substitution of residues needed for actin binding
Utrophin • Ubiquitous Dystrophin • Two isoforms • Utrophin A found in skeletal muscle • Utrophin B found in vascular endothelium • Interest in replacing defective dystrophin with utrophin A • Utrophin and Dystrophin ABDs share a 72% sequence identity and both associate with members of DAPC • Both are antiparalleldimers of two ABDs each made of calponin domains CH1 and CH2, and are dumbbell shaped • *Utrophin performs function of dystrophin in fetal and developing muscle fibers seen by high levels during development in sarcolemma
F C D B G E A C-Terminal Utrophin Dystrophin I G C A E N-Terminall F
Within dystrophin and utrophin dimers, domain swapping of CH-domains between monomer chains A and B result in CH1 –CH2 interface is very similar to that of fimbrin ABD • Not sure if this occurs in vivo or is just a product of crystallization because utrophin is found monomeric in solution and dystrophin in a monomer- dimer equilibrium • *Differences lie in the loops connecting the helices
Dystrophin Utrophin Fimbrin BCH2 ACH1 BCH2 CH2 CH1 ACH1 ACH2 ACH2 BCH1 BCH1
Studies have enabled to propose likely molecular model for binding of utrophin CH domain and compared to dystrophin ABD • Biochemical characteristics of these have been extensively studied • Negative staining and cryo-EM showed uniform binding of F-actin by utrophin and binds to actin as a 1:1 complex • EM showed that dystrophin decorated F-actin uniformly without crosslinking filaments and bound to actin as 2:1 (dys:act)
Utrophin Actin Binding Sites ABS1 ABS1 34-43 ABS2 105-132 ABS3 147-163 ABS2 ABS3
CH2 Dystrophin Utrophin CH1
Quick Background • Been known that DMD patients have greater damage in fast fibers than in slow counterparts • Possible explanation comes from observation that utrophin is expressed in extrasynaptic regions of these fibers and thus protect against muscle damage • In order to show utrophin regulator in slow myogenic program the stimulation of slow muscle phenotype by functional overload results in greater expression of Utrophin A
Utrophin tests • Studies on mdxmouse show elevation of utrophin levels in dystrophin muscle fibers can restore sarcolemmal expression of DAPC members and alleviate pathology • Done by germline gene transfer and somatic gene transfer- dangerous because trigger adverse immune response • However increase of endogenous utrophin using pharmocological intervention is appealing because of its systematic administration, lack of detrimental effects, and would be effective for all DMD patients regardless of subset
Challenge of Utrophin • Main difference is in the contrast of expression patterns and length • Dystrophin runs entire length • Utrophin is confined to myotendinous and neuromuscular junction (NMJ) • Stimulate expression of utrophin at appropriate levels along entire sarcolemma
Utrophin Mechanism of transcription • Important to understand utrophin A expression at NMJ to see how utrophin can function the entire length of sarcolemma • The entire biochemistry is pretty in depth so I will go into the three most important parts • Calcineurin effect on nuclear facot of activated T cells (NFAT) • Heregulin activation of GABPα and GABPβ • neuronal nitric oxide synthase(nNOS)
Calcineurin and NFAT • Hypothesized that because Ca2+ dependent and calmodulindepedendentcalcineurin is important regulator of slow myogenic program, it is a regulator of utrophin expression • Increases mRNA levels in slow muscle fibers of mouse • Inhibition decreases mRNA levels in slow muscle fibers • More work is needed to substantiate but believed that calcineurin exerts effect on nuclear factor of activated T cells (NFAT) • Utrophin A promoter region contains NFAT binding site and overexpression of NFAT induces transcription of utrophin A • stimulation of slow myogenic program and increased utrophin levels through activation of calcineurin-NFAT might be appropriate therapy to protect against degeneration of dystrophin muscle fibers
Heregulin • Nerve derived growth factor • Can stimulate utrophin transcription through GABPα and GABPβ and binding to N-box motif • Study show that administration of small peptide region of heregulin ectodomain to mdx mice was shown to increase utrophin expression and improve dystrophin phenotype • *Three fold increase in utrophin levels after 4 week old mdx mice treated for 3 months • **the expression of utrophin found throughout the entire length of sarcolemma • ***reduction of muscle degeneration and inflammation and decreased susceptibilitly to damage induced by lengthening contractions • Note- muscle fibers not as dramatic as somatic-gene transfer of utrophin but this outweighed due to advantages of systemic drug therapy over genetic
Neuronal Nitric Oxide Synthase and L-Arganine • nNOS- enzyme that catalyzes production of potent signaling molecule nitric oxide • In dystrophic mice nNOS considerably reduced and leaks from disruption of DAPC • Overexpression of nNOStransgene in mdx mice reduced extent of pathology • L-Arganine- substrate for nNOS, also increased utrophin expression in mdxmcie • Showed reduced necrosis and contractile-induced damage • Increase varies but reported significant 2 and 3 fold increased
Conclusion to Utrophin Therapies • Side effect damage from calcineurin-NFAT signaling can not be overlooked because cardiac hypertrophy is known to be induced by calcineurin • However, interestingly corticosteroid deflazacort (mentioned earlier) stimulates calcineurin-NFAT pathway which have showed beneficial effects • Heregulin peptide is plausible treatment but also need to assess long-term toxicity effects and tissue specificity • Fewest obstacles is nNOS because NO regulation is used for other disease but will be difficult to target it to skeletal muscle because it plays a role in most tissue • Although these might induce side-effects, for now they are outweighed by need for effective therapies
Utrophin-Myostatin • Time for using utrophin based therapy to treat DMD has not yet arrived but significant progress has been made • However, utrophin-based therapy should not be used alone and should be used in combination with block of Myostatin • This should hopefully significantly improve quality and duration of life of people affected
Myostatin • Member of transforming growth factor-β (TGF β) • Strong negative regulator of muscle growth • With this protein inhibited muscles do not stop growing • Myostatin knock-out mice 2-3 times larger muscles than WT • Mutations have been seen in cattle, sheep dogs, and humans • Myostatin inhibitors being searched for treatment of muscle dystrophies
Liam ROOSEVELT PARK, Mich. -- Liam Hoekstra was hanging upside down by his feet when he performed an inverted sit-up, his shirt falling away to expose rippled abdominal muscles.It was a display of raw power one might expect to see from an Olympic gymnast.Liam is 19 months old.But this precocious, 22-pound boy with coffee-colored skin, curly hair and washboard abs is far from a typical toddler."He could do the iron cross when he was 5 months old," said his adoptive mother, Dana Hoekstra of Roosevelt Park. She was referring to a difficult gymnastics move in which a male athlete suspends himself by his arms between two hanging rings, forming the shape of a cross. http://awurl.com/
Myostatin • belongs to activin class of molecules because it binds to activin type II receptors, ActRIIB and ActRIIA and activin inhibitor follistatin(fst) • Signals through activin type I receptor (Alk4) • Signals through TGF-β type I receptor (Alk5) • Regulated by antagonists like decorin, GASP-1, and Fst-type molecules • Fst-like 3 (Fstl3) and isoforms Fst288 and Fst315 • Fst binds to activin with a greater affinity than to myostatin
Myostatin Structure • Displays traditional TGF-β family hand shaped architecture • Each monomer consists of four curved beta strands- “fingers” • A cystine know motif- “palm” • Major helix- “wrist” • Two monomers come together palm to palm in an anti-parallel direction and form an intermolecular disulfide bond
Myostatin typical hand architecture 4 beta strands-fingers Cystine knot motif- palm Helix- Wrist
Prehelix shape determines Alk5 signaling • Myostatin can bind to Alk5, TGF-β type I receptors, and Alk4, activin type I receptors • Compared prehelix region between Activin and found big differences • Activin A has glycine and serine residues causing to be more flexible • Myostatin has large hydrophobic residues • Myostatin has very similar prehelix region shape to TGF-β3 even though amino acids are different, TGF-β3 also has high affinity to ALK5 • Conclusion the prehelix loop allows signaling through Alk5 and does not matter on amino acids but more on shape due to van der Walls forces • Switching prehelix region of activin A with that of myostatin allows lots of signaling through Alk5 – eight fold
Myostatinn Prehelix domain Utrophin
follistatin • Multidomain protein consisting of N-terminal domain and three subsequent Fst domains • Binds to heprain which localizes it to cell surfaces and facilitates endocytosis of Fst-bound ligands • Antagonist and strongly inhibits activin A, close family member of myostatin • Inhibit signaling by completely surrounding the ligand with two molecules, blocking all four receptor binding sites
Heparin • follistatinis known to bind to heparin • Implications in localizations and cellular endocytosis, because this allows molecules to bind to cell surfaces • Myostatin-follistatincomplex are very electropositive • The FSD1 herpain binding sites are on both follistatinmolecules • Myostatin has a high polar surface potential with the bottom • The highly basic surface of myostatin may hinder ability of follistatinto bind, because it brings together two electropositive surfaces • Could explain why affinity for follistatinis higher in activin than myostatin • However! Affinity of heparin to the myostatin/follistatincomplex is increased
Biological implications to Heparin binding • Stabilize the myostatin complex by bridging both Fst molecules and balancing the electrostatic surface charge • Heparin bound Fst may have increased affinity for myostatin, as heparin would diminish the putative electrostatic repulsion of myostatin and Fst coming together • Lead to more preferred binding of cell surface bound Fst to myostatin over activin A • With increase binding to myostatin a mechanism to easily inhibit myostatin can be found and used in DMD patients