Download
1 / 10
100 likes | 622 Views
TRANSVERSE In a transverse lie, a fetus lies horizizontally in the pelvis so that the longest fetal axis is perpendicular to that of the mother. The presenting part is usually one of the shoulders (acromion process), an iliac crest, a hand, or an elbow. Types of Malpresentation.

E N D
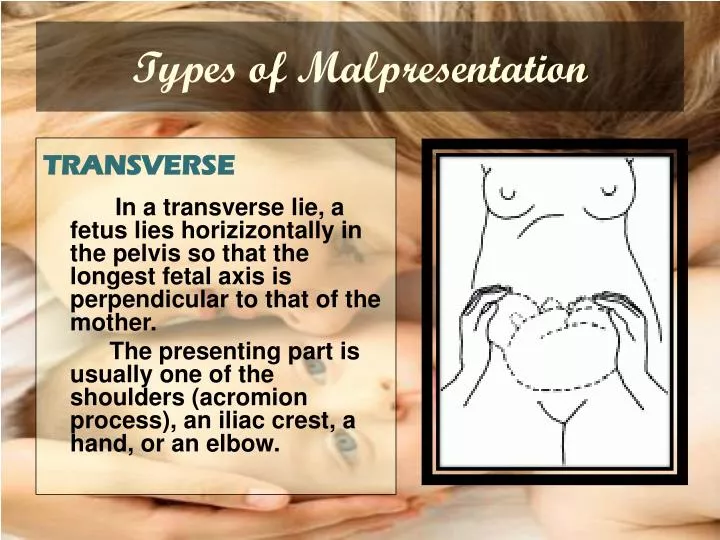
TRANSVERSE In a transverse lie, a fetus lies horizizontally in the pelvis so that the longest fetal axis is perpendicular to that of the mother. The presenting part is usually one of the shoulders (acromion process), an iliac crest, a hand, or an elbow. Types of Malpresentation
Management • If an infant is preterm and smaller than usual, an attempt to turn the fetus to a horizontal lie may be made. • Most infants in transverse lie must be born by cesarean birth, however, because they cannot be turned and cannot be born normally form this “wedged” position.
SINCIPUT The sinciput presentation occurs when the larger diameter of the fetal head is presented. Labor progress is slowed with slower descent of the fetal head. FACE The face presentation is caused by hyper-extension of the fetal head so that neither the occiput nor the sinciput is palpable on vaginal examination. Types of Malpresentation
In the chin-anteriorposition prolonged labor is common. Descent and delivery of the head by flexion may occur. In the chin-posterior position, however, the fully extended head is blocked by the sacrum. This prevents descent and labor is arrested. Management
Chin-Anterior Position If the cervix is fully dilated: Allow to proceed with normal childbirth; If there is slow progress and no sign of obstruction, augment labor with oxytocin; If descent is unsatisfactory, deliver by forceps. If the cervix is not fully dilated and there are no signs of obstruction: augment labor with oxytocin. Chin-Posterior Position If the cervix is fully dilated: Deliver by caesarean section. If the cervix is not fully dilated Monitor descent, rotation and progress. If there are signs of obstruction, deliver by caesarean section. *Do not perform vacuum extraction for face presentation. Management
BROW The brow presentation is caused by partial extension of the fetal head so that the occiput is higher than the sinciput. MGT: If the fetus is alive or dead, deliver by caesarean section. *Do not deliver brow presentation by vacuum extraction, outlet forceps or symphysiotomy. Types of Malpresentation
Nursing Care of Clients with Malpresentations • Observe closely for abnormal labor patterns. • Monitor fetal heart beat and contractions continuously. • Anticipate forceps-assisted birth. • Anticipate cesarean birth for incomplete breech or shoulder presentation. • Be prepared for childbirth emergencies such as cesarean section, forceps-assisted delivery, and neonatal-resuscitation. • Position pt. in Trendelenburg or knee-chest position. • Manually raise the presenting part aseptically
Anxiety • Provide client and family teaching, • Be available to client for listening and talking • Provide client support and encouragement. • Encourage client to acknowledge and express feelings. • Encourage breathing exercises to relieve anxiety. Fear • Provide client and family teaching, • Note for degree of incapacitation. • Stay with the client or make arrangements to have someone else be there. • Provide opportunity for questions and answer honestly. • Explain procedures within level of client’s ability to understand and handle.
Risk for Injury • Observe closely for abnormal labor patterns. • Monitor fetal heart beat and contractions continuously • Be prepared for childbirth emergencies such as cesarean section, forceps-assisted delivery, and neonatal-resuscitation. • Maintain sterility of equipments • Anticipate forceps-assisted birth. • Anticipate cesarean birth for incomplete breech or shoulder presentation. Risk for infection • Stress proper hand washing techniques of all caregivers. • Maintain sterile technique. • Cleanse incision site daily and prn. • Change dressings as needed. • Encourage early ambulation, deep breathing, coughing, and position change.