Download

1 / 49
620 likes | 1.89k Views
Skeletal Muscle Relaxants. Drug List. Muscle. Nerve. Nerve. Presynaptic terminal Sarcolemma Synaptic vesicles Acetylcholine receptors Mitchondrion. Na+ . ACh. Neuromuscular Junction. Na+ . Neuromuscular Blocking Drugs. ACh. Competitive Tubocurarine Gallamine Pancuronium

E N D
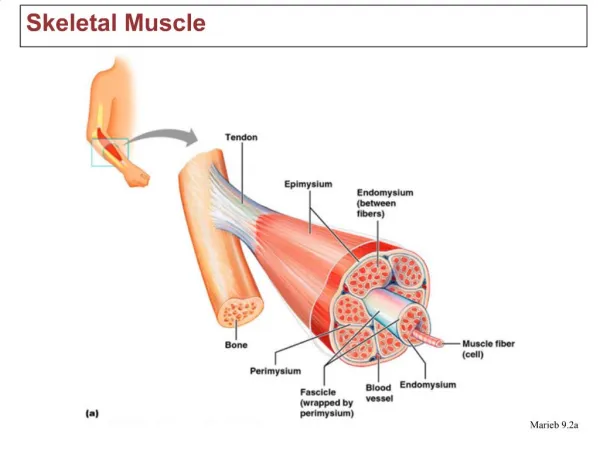
Muscle Nerve Nerve
Presynaptic terminal Sarcolemma Synaptic vesicles Acetylcholine receptors Mitchondrion
Na+ ACh Neuromuscular Junction Na+ Neuromuscular Blocking Drugs ACh Competitive Tubocurarine Gallamine Pancuronium Vecuronium Atracurium Rocuronium Depolarizing Suxamethonium δ α γ α β
Muscle Relaxants What are they used for? • Facilitate intubation of the trachea • Facilitate mechanical ventilation • Optimized surgical working conditions • Treatment of Convulsions / seizures
Also used for • Muscle spasticity • Muscle Spasms What are spasticity and spasms? Spasticity can be described as involuntary muscle stiffness and spasms as involuntary muscle contractions. Any muscle can be affected but spasticity and spasms tend to predominantly affect a person's limbs or trunk.
Definition of muscle spasm • Increased muscle tone • together with muscle weakness It is often associated with cerebral palsy, multiple sclerosis, and stroke.
Causes of Muscle Spasms • Seen after musculoskeletal injury and inflammation • Involve afferent nociceptive input from damaged area • Excitation of alpha motor outflow • Tonic contraction of affected muscle • Build up of pain-mediating metabolites
Levels of Muscle Relaxant Intervention • Spinal Cord • NEUROMUSCULAR Junction • Muscle Cells
Muscle Relaxants Definition: Drugs which relax skeletal muscles by acting at the neuromuscular junction • Depolarizing muscle relaxant Succinylcholine • Nondepolarizing muscle relaxants Short acting Intermediate acting Long acting
They can also be called • Antagonist(nondepolarizing) neuromuscular blocking drugs prevent access of acetylcholine to its NM receptorand prevent depolarization of the motor end plate (d-tubocurarine) • Agonist(depolarizing) neuromuscular blocking drugs produce excessive depolarization of the motor end plate by causing excessive stimulation of the NM receptor (Succinylcholine)
Succinylcholine What is the mechanism of action? • Physically resemble Ach • Act as acetylcholine receptor agonist • Not metabolized locally at NMJ • Metabolized by pseudocholinesterase in plasma • Depolarizing action persists > Ach • Continuous end-plate depolarization causes muscle relaxation
Succinylcholine • What is the clinical use of succinylcholine? • Most often used to facilitate intubation • Onset 30-60 seconds, duration 5-10 minutes
Succinylcholine What is phase I neuromuscular blockade? Repetitive firing and release of neurotransmitter. Acetylcholine receptors remain open. Preceded by fasciculations. What is phase II neuromuscular blockade? Postjunctionalmembrane does not respond to ACh even when resting membrane potential is restored i.e. Desensitisation blockade or Phase II block.
Succinylcholine Does it have side effects? • Cardiovascular • Fasciculation • Muscle pain • Increase intraocular pressure • Increase intragastric pressure • Increase intracranial pressure • Hyperkalemia • Malignant hyperthermia
Nondepolarizing Muscle Relaxants Long acting Pancuronium Intermediate acting Atracurium Vecuronium Rocuronium Cisatracurium Short acting Mivacurium Mechanism of Action All bind nicotinic Ach receptors and competitively block Acetylcholine, thereby preventing muscle contraction i.e. They are competitive antagonists
Tubocurarine • This was the first muscle relaxant used clinically • Therapeutic Use: Adjuvant drugs in surgical anesthesia • Pharmacology: Must be given by injection because they are poorly absorbed orally. Do not cross the BBB. • Elimination: Generally excreted unchanged (i.e. not metabolized). • Adverse Effects:Tubocurarine causes release of histamine from mast cells – decrease in blood pressure, bronchospasms, skin wheals. • Drug interaction: Competes with succinylcholine for it’s the end plate depolarizing effect.
Pancuronium • It is an Aminosteroidcompound • Onset 3-5 minutes, duration 60-90 minutes • Elimination mainly by kidney (85%), liver (15%) • Side effects : hypertension, tachycardia, dysrhythmia
Vecuronium • Analogue of pancuronium • Much less vagolytic effect and shorter duration than pancuronium • Onset 3-5 minutes duration 20-35 minutes • Elimination 40% by kidney, 60% by liver
Rocuronium • Analogue of vecuronium • Rapid onset 1-2 minutes, duration 20-35 minutes • Onset of action similar to that of succinylcholine • Intubating dose 0.6 mg/kg • Elimination primarily by liver, slightly by kidney
Atracurium Metabolized by • Ester hydrolysis • Hofmann elimination(spontaneous degradation in plasma and tissue at normal body pH and temperature) Onset 3-5 minutes, duration 25-35 minutes Side effects: • histamine release causing hypotension, tachycardia, bronchospasm • Laudanosinetoxicity (Laudanosine is a metabolite of atracurium and cisatracurium. It decreases seizure threshold and this it can induce seizures, however, such concentrations are unlikely to be produced at therapeutic doses)
Cisatracurium • Isomer of atracurium • Metabolized by Hofmann elimination • Onset 3-5 minutes, duration 20-35 minutes • Minimal cardiovascular side effects • Much less laudanosine produced
Mivacurium • Has the shortest duration of action of all nondepolarizing muscle relaxants • Onset of action is significantly slower • Use of a larger dose to speed the onset can be associated with profound histamine release leading to hypotension, flushing, and bronchospasm. • Clearance of mivacuriumby plasma cholinesterase is rapid and independent of the liver or kidney. • Mivacuriumis no longer in widespread clinical use. It is an investigational ultra-short-acting
Drug Interactions • Cholinesterase Inhibitors decrease the effectiveness of nondepolarizingagents • Aminoglycoside antibiotics increase action of nondepolarizingdrugs • Calcium channel blockers increase the actions of nondepolarizing drugs • Inhalational anesthetics enhance neuromuscular blockade by nondepolarizing drugs
Reversal of Neuromuscular Blockade Why do we need to reverse the effect of neuromuscular blockers? Because they paralyze the muscles. Once the surgery is over, the muscles need to work again. Goal:re-establishment of spontaneous respiration and the ability to protect airway from aspiration
Reversal of Neuromuscular Blockadeby Anticholinesterases Effectiveness of anticholinesterases depends on the degree of recovery present when they are administered Anticholinesterases Neostigmine • Onset 3-5 minutes, elimination halflife 77 minutes Pyridostigmine Edrophonium
What is the mechanism of action? • Inhibiting activity of acetylcholineesterase • More Ach available at NMJ, compete for sites on nicotinic cholinergic receptors • Action at muscarinic cholinergic receptor • Bradycardia • Hypersecretion • Increased intestinal tone
What do we do about side effects? • Muscarinic side effects are minimized by anticholinergic agents • Atropine • Dose 0.01-0.02 mg/kg • Scopolamine • glycopyrrolate
Baclofen • Mechanism of action: GABABagonist • Clinical effects:decreased hyperreflexia; reduced painful spasms; reduced anxiety
Baclofen • Adverse effects: weakness, sedation, hypotonia, ataxia, confusion, fatigue, nausea, liver toxicity • Chronic effects: rapid withdrawal may cause seizures, confusion, increased spasticity • Route of administration: oral, intrathecal
Tizanidineand Clonidine • Mechanism of action: alpha-2 receptor agonist • Clinical effects: reduced tone, spasm frequency, and hyperreflexia
Tizanidineand Clonidine • Adverse effects: drowsiness, dizziness, dry mouth, orthostatic hypotension • Chronic effects: rebound hypertension with rapid withdrawal • Route of administration: oral, transdermal patch (Clonidine)
Diazepam Lorazepam (Ativan) Clonazepam Clorazepate Ketazolam Tetrazepam Benzodiazepines
Diazepam (Valium) • Mechanism of action: enhance GABAA activity (chloride channels) • Clinical effects: decreased resistance to passive joint range of motion (ROM); decreased hyperreflexia; reduced painful spasms; sedation; reduced anxiety
Diazepam (Valium) • Adverse effects: sedation, weakness, hypotension, memory impairment, ataxia, confusion, depression • Chronic effects: dependency, withdrawal, and tolerance possible • Routes of administration: oral, intravenous, rectal
Peripheraly acting spasmolytic drugsDantrolene Mechanism of action: Dantrolene reduces skeletal muscle strength by interfering with excitation-contraction coupling in the muscle fibers Normal contraction involves release of calcium from its stores in the sarcoplasmic reticulum through a calcium channel Dantrolene interferes with the release of calcium through this sarcoplasmic reticulum calcium channel.
Dantrolene: Indications: 1- Muscle spasticity 2- Malignant hyperthermia:
Botulinum Toxin (Botox) • Enters the pre-synaptic terminal and binds to acetylcholine • Inhibits acetlycholine from entering the synaptic cleft • Toxin serves as a block at the neuromuscular junction • Can be administered to a specific muscle or group via local injection
Botox • Used in treatment of patients with focal dystonia as found in stroke and spinal cord lesions • Used to restore volitional motor control thus increasing use of extremities and improving function, mobility and opportunities to participate in meaningful occupations • Prevention of joint contraction and fixation