Download
1 / 22
250 likes | 509 Views
Research utilization in policy development. Sripen Tantivess International Health Policy Program A presentation at the Health Systems Research Institute 25 th July 2008. What to be addressed:. Policies. Research. Actions. Bridging research and policy (R2P). Open to subjective judgment

E N D
Research utilization in policy development Sripen Tantivess International Health Policy Program A presentation at the Health Systems Research Institute 25th July 2008
What to be addressed: Policies Research Actions Bridging research and policy (R2P)
Open to subjective judgment (Politically-oriented) Scientific rigour (Sauerborn R, S Nitayarumphong, A Gerhardus. Strategies to enhance the use of health systems research for health sector reform. 1999;4(12):827-35)
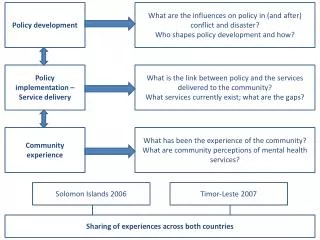
Research-policy nexus Research scientific evidence policy decisions Links between policy and research communities: Political context: Networks, relationships, power, competing discourses, trust, etc. Political and econ. structures & interests; institutional pressures; cultural differences; preferences for incremental VS radical changes, etc. Credibility of evidence: Degree to which it challenges received wisdom; research methods; credibility of researcher; simplicity of message; how it is communicated, etc. (Young, J. Research and policy: parallel universe? In Annual Report 2002/3. Oversea Development Institute, London, 2003)
‘Greater attention to health policy analysis will help to assure that the results from research penetrate into policy and practice’ (Walt, Gill. How far does research influence policy? European Journal of Public Health 1994; 4:233-235) ‘Health policy analysis can help to explain why certain health issues receive political attention, and other do not, such as by enabling identification of which stakeholders may support or resist policy reforms, and why.’ (Gilson, Lucy et al. Future directions for health policy analysis: a tribute to the work of Prof Gill Walt. Health Policy and Planning, forthcoming 2008)
Examples of health policies • Antiretroviral therapy shall be provided to all clinically-eligible patients • Smoking is prohibited in public facilities • The government’s priority are health promotion and disease prevention, rather than treatment • Car driver and passengers in front seats must have seatbelt fastened all the time • Ten million baht will be allocated to information & education programs concerning non-communicable diseases in 2009
Context Actors Content Process Basic framework for policy analysis: the Policy Triangle (Walt, G and L Gilson. Reforming the health sector in developing countries: the central role of policy analysis. Health Policy and Planning 1994; 9: 353-370)
CONTEXT Systemic factors which may have an effect on policy • Situational factors (transient, impermanent), e.g. outbreak, war, economic recession, droughts • Structural factors (relatively unchanging elements), e.g. political system, type of economy, wealth, demographic features, technological advance • Cultural factors, e.g. religious, hierarchies, social norms • International or exogenous factors (Leichter, Howard M. 1979. A comparative approach to policy analysis: health care policy in four nations. Cambridge: Cambridge University Press.)
Sun Tzu: The Art of War • If you know the enemy and know yourself, you need not fear the result of a hundred battles. • If you know yourself but not the enemy, for every victory gained you will also suffer a defeat. • If you know neither the enemy nor yourself, you will succumb in every battle. Knowing what?
Stakeholder analysis High • Government party Q I Q IV • Health ministry • Medical council • NGOs POWER • Physicians RESOURCES Q II Q III • Consumers • Hospitals • Drug stores • Drug industry Low POSITION Against Support Loss – INTEREST – Gain
‘Knowing who the key actors are, their knowledge, interests, positions, alliances, and importance related to the policy allows policy makers and managers to interact more effectively with key stakeholders and increase support for a given policy or program.’ (Schmeer, K. Guidelines for Conducting a Stakeholder Analysis. Bethesda, MD: Partnerships for Health Reform, Abt Associates Inc., 1999)
Actor networks(clusters of actors in particular policy domains) • A determinant of policy success or failure • Increasingly important in the globalization world, where policy processes are complex • Network members are interdependent • Common interests, objectives and ideals • Resource sharing and exchanges • Resource mobilization from outside
(Sauerborn R, S Nitayarumphong, A Gerhardus. Strategies to enhance the use of health systems research for health sector reform. 1999;4(12):827-35)
(Sauerborn R, S Nitayarumphong, A Gerhardus. Strategies to enhance the use of health systems research for health sector reform. 1999;4(12):827-35)
Policy learning (policy transfer) model:acquiring knowledge for policymaking • Policy can be transferred across time and place • Voluntary – Coercive • Consciously – Unconsciously • Learned objects: ideologies, ideas, goals, objectives, strategies, instruments • Learning process: consideration, anticipation, assessment, inspiration, adaptation, adoption, rejection ‘In most situations, policy makers tend not to invest their time and resources in seeking fresh knowledge, i.e. commissioning research to inform policies, but to search for lessons from their own organisations including past experiences, neighbouring agencies and also foreign countries’ (Rose 1991)
Instrumental use: research findings directly drive or define policy. • Mobilisation of support [supportive evidence]: research findings provide persuasive evidence to back ongoing and proposed policy activities or raise awareness and support for new policy-making. • Conceptual use: research leads to new ideas and language that influence the nature and substance of policy discourse. • Redefining/wider influence: research impact that leads to a wide change or transformation of accepted beliefs and practices. Nature of policy influence of health research: Available at: http://www.biomedcentral.com/content/pdf/1472-6963-6-134.pdf
Construction-interpretation-perceptions and power of discourses • It is not external events that cause policy change, but how these events are perceived, interpreted and articulated (Hajer 1993). • Language or discourse may shape the policy agenda, and how problems and solutions are understood (Kingdon 1984). Actors are not value-free. They respond to issues, problems and policies in the ways to address what they perceive and construct. • ‘By weaving a selection of facts, beliefs and values into a plausible prescriptive narrative, these policy frames, or storylines, allow actors and publics to reduce the complexity of policy problems, ascribe meaning to problems and events and crudely assess possible policy alternatives’ (Juillet 2007). • ‘By dramatising or downplaying the problem and by declaring what is at stake, these descriptions help to push an issue onto the front burners of policymaking or result in officials’ stubborn inaction and neglect.’ (Rochefort DA., and RW Cobb. 1994)
Issue definitions – policy Image • Is it a normal phenomenon or a problem? “Problematising” • What sort of problem? Health or non-health, public health or biomedical (medicalisation) • Severity: magnitude, dissemination, urgency and implications • Problem of whom? • Construction of causality and afflicted population who should be responsible for it? • Is this an appropriate solution? How ‘appropriateness’ is justified?
Practical criteria for selection of policy options • Political desirability • Social acceptability • Technical & management feasibility • Affordability & benefits What are the policymakers’ and key stakeholders’ perceptions towards quality of research and policy recommendations?
Strategies for policy change • Aim: to strengthen/mobilise supportive actors and undermine/ demobilise the opposition • What to be managed? • Position (Proposal): alter particular components of a policy • Power: affect the distribution of political resources (money, information, image, expertise) across groups • Players (actors): recruiting and dividing • Perception: address the perceptions of actors towards problems and solutions (Roberts, MJ et al (2004) quoted in Buse K et al. Making Health Policy. Berkshire: Open University Press, 2005)
Key messages • The role of scientific evidence is variable, depending on the stage of the policymaking process at which it is introduced. • The relationship between any given body of evidence and public policy depends on the dominance of the advocacy coalition that has appropriated it. • Policymaking is a social process and evidence is socially constructed. • Analyzing and promoting certain policy options is a process of facilitating conversations and dialogue between different participants in the policy process. • Proponents of healthy public policy need to analyze discourse, identify different and competing policy frames, and promote dialogue between members of the many communities that will feel the impacts of policy and program change. (Fafard P. Evidence and Healthy Public Policy: Insights from Health and Political Sciences. Ottawa: National Collaborating Centre for Healthy Public Policy, 2008)
‘If researchers and policy analysts wish to have a significant impact on policy, they generally must abandon the role of neutral technician and instead adopt that of an advocate.’ (Flora CB, JL. Flora, F Campana, E Fernández-Baca. The Advocacy Coalition Framework: A Theoretical Frame for SANREM to Address Policy Change and Learning. http://www.mtnforum.org/oldocs/970.pdf)