Download
1 / 27
270 likes | 407 Views
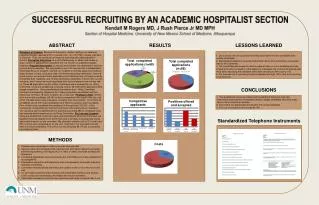
a. Effects of Advanced Care Discussion in Patient Care Conferences at a Long-Term Care Facility. Karen M. Zagrocki, DNP, CRNP Mario J. Fatigati, MD, FACP, CMD John J. Kane Regional Center, Scott Township Pittsburgh, PA. Speaker Disclosures.

E N D
a Effects of Advanced Care Discussion in Patient Care Conferences at a Long-Term Care Facility Karen M. Zagrocki, DNP, CRNP Mario J. Fatigati, MD, FACP, CMD John J. Kane Regional Center, Scott Township Pittsburgh, PA
Speaker Disclosures Karen M. Zagrocki, DNP, CRNP, has disclosed that she has no relevant financial relationship(s). Mario J. Fatigati, MD, has disclosed that he has no relevant financial relationship(s).
Acknowledgements John J. Kane Regional Center, Pittsburgh, PA • Special recognition and thanks to the residents, families, staff, and administration for their support and participation in this quality improvement initiative. Jewish Health Care Foundation, Pittsburgh, PA • Grant Title: Alvin Rogal Research Award in Safety and Quality Improvement
Learning Objectives By the end of the session, participants will be able to: • Know and understand the components of an advanced care planning educational intervention for a multidisciplinary team • Know and understand the components of advanced care planning discussion intervention in patient care conferences • Identify the benefits and outcomes of advanced care discussion in patient care conferences at a long term care facility
Introduction • Hospitalizations and hospital transfers are common occurrences for residents with high risk mortality in nursing home facilities • ↑ Hospitalizations in last six months of life (Lamberg et al., 2005) • Leads to possible: • Uncomfortable medical interventions • Questionable benefits • Poor prognosis for survival • Decreased quality end-of-life care • Considerable burden • Increased health care expenditures (Ahearn, Jackson, McLlmoyle, & Weatherburn, 2010; Lamberg, Person, Kiely, & Mitchell, 2005; Ouslander, et al., 2010)
Introduction • 67-76% hospitalizations are avoidable • Ongoing assessment • Identification of changes in physical conditions • Better advance care planning (ACP) (Lamb, Tappen, Diaz, Herndon, & Ouslander, 2011; Ouslander, et al., 2010)
Scope of the Problem • Advanced care discussions • Often delayed • Life-threatening illness • Imminent death • Time limitations/restraints of clinicians • Emotional readiness (Bravo, Dubois, & Wagneur, 2008; Lamberg et al., 2005) • CPR wishes completed regularly • Per admission requirements and emergent changes in health condition • Ongoing comprehensive documentation goals of care limited • Each discipline completed independently • Shared communication limited
Scope of the Problem • POLST form completion • Regularly documented residents’ cardiopulmonary resuscitation wishes • But often inconsistently completed comprehensive documentation regarding end-of-life preferences’ • Palliative/hospice services underutilized (Ahearn et al., 2010; Hickman, et al., 2010; Lamberg et al., 2005; Levy, Morris, & Kramer, 2008)
Goals: Improving Advanced Care Planning • Use multidisciplinary approach • Provide ACP education for multidisciplinary team • Improve ACP discussion and documentation • Provide shared, ongoing communication among all disciplines, families and residents • Improve comprehensive completion of POLST form • Identify residents goals of care to ensure end-of-life wishes are identified and respected
Our Question Does the integration of ACP discussion along with review of POLST form at patient care conferences by the multidisciplinary team at a long-term care facility decrease unnecessary hospitalizations, increase advance directive documentation, hospice consultations and comfort measures only (CMO) orders?
Quality Improvement Initiative • ACP Educational training intervention • ACP Discussion Intervention • Patient care conferences • Conducted in accordance to federal OBRA regulations for new resident admissions and established long term care residents • Based on Minimum Data Set (MDS) 3.0 • Conferences evaluated over six month period and compared to previous year six month period
Quality Improvement Initiative • Outcomes assessed: • Documentation of ACP discussion • Nursing/social services and clinicians • Modification of end-of-life preferences’ and comfort measure orders (POLST form) • Hospitalizations/emergency room visits • Hospice consultations
ACP Educational Training Intervention • Two day, two hour education program • MDS nurses, nursing supervisors, social services and dietitians • Educational content included: • Conducting advanced care discussions • Components of POLST Paradigm • Hospice criteria, enrollment, and services • Identification of high risk mortality residents • Using Flacker Mortality Risk Index • EPrognosis [Website program]. (2012).Retrieved from http://www.eprognosis.org/2011/05/flacker-2-index.html#
ACP Discussion Intervention • Interdisciplinary team role • Identify prior to each patient care conference • 65 years and older • Meets criteria for high risk mortality or • Documented decline in status based on significant change in status criteria • Facilitate ACP discussion at scheduled patient care conferences • Document end-of-life preferences/changes using ACP worksheet tool • Notify attending physician/nurse practitioner of discussion
ACP Discussion Intervention • Physician/Nurse Practitioner role • Requested to review/update POLST form • Document ACP discussion • Consult hospice if appropriate
Results Advanced Care Discussion
Effect of ACP Discussion and Hospitalizations/Emergency Room Visits
Implications of Education and Clinical Practice • Collaborative multidisciplinary approach helps to ensure resident’s end-of-life preferences are implemented • Shared communication improves quality end-of-life • Ongoing, frequent ACP discussion ensures resident goals of care • Improving advanced care discussion and documentation • Provides specific treatment plan for resident’s goals of care • Increases comfort care for residents
Conclusion • Integration of ACP discussion and review of POLST Paradigm in patient care conferences: • Increases advanced care documentation • Increases comfort measure only orders • Increases hospice utilization • Potentially decreases unnecessary hospitalizations
References Ahearn, D. J., Jackson, T. B., McLlmoyle, J., & Weatherburn, A. J. (2010). Improving end of life care for nursing home residents: an analysis of hospital mortality and readmission. Postgrad Medical Journal, 86, 131-135. Bravo, G., Dubois, M. F., & Wagneur, B. (2008). Assessing the effectiveness of interventions to promote advance directives among older adults: A systematic review and multi-level analysis. Social Science & Medicine, 67, 1122-1132. EPrognosis [Website program]. (2012). Retrieved from http://www.eprognosis.org/2011/05/flacker-2-index.html# Hickman, S. E., Nelson, C. A., Perrin, N. A., Moss, A. H., Hammes, B. J., & Tolle, S. W. (2010). A comparison of methods to communicate treatment preferences in nursing facilities: Traditional practices versus the physicians orders for life-sustaining treatment program. Journal of American Geriatric Society, 58(7), 1241-1248. Lamb, G., Tappen, R., Diaz, S., Herndon, L., & Ouslander, J. G. (2011). Avoidability of hospital transfers of nursing home residents: Perspectives of frontline staff. Journal of American Geriatric Society, 59(9), 1665-1672. Lamberg, J. L., Person, C. J., Kiely, D. K., & Mitchell, S. L. (2005). Decisions to hospitalize nursing home residents dying with advanced dementia. Journal of American Geriatric Society, 53(8), 1396-1401 Levy, C., Morris, M., & Kramer, A. (2008). Improving end-of-life outcomes in nursing homes by targeting residents at high-risk of mortality for palliative care: Program description and evaluation. Journal of Palliative Medicine, 11, 217-225. Ouslander, J. G., Lamb, G., Perloe, M., Givens, J. H., Kluge, L., Rutland, T.,...Saliba, D. (2010). Potentially avoidable hospitalizations of nursing home residents: Frequency, causes, and costs. Journal of American Geriatric Society, 58(4), 627-635.