Download
1 / 40
400 likes | 602 Views
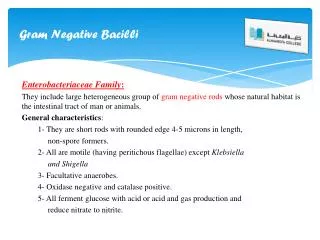
Resistant Gram-Negative Bacilli ESBLs and Other Bad Bugs. David P. Dooley, FACP UTHSC-San Antonio Audie Murphy VA Hospital San Antonio, TX. Resistant GNB The Problem. Still common in their nich é s; level prevalance of GNBs, but resistance rising.

E N D
Resistant Gram-Negative BacilliESBLs and Other Bad Bugs David P. Dooley, FACP UTHSC-San Antonio Audie Murphy VA Hospital San Antonio, TX
Resistant GNBThe Problem • Still common in their nichés; level prevalance of GNBs, but resistance rising
Results of intensive care unit surveillance revealing percentages of gram-positive (Gram Pos) and gram-negative (Gram Neg) pathogens associated with pneumonia, urinary tract infection (UTI), surgical site infection (SSI), and bloodstream infection (BSI)—National Nosocomial Infections Surveillance system, 1986–2003.
Results of intensive care unit surveillance for the proportion of selected gram-negative organisms reported for pneumonia from the National Nosocomial Infections Surveillance system, 1986–2003. Gaynes R CID 2005 (CDC)
Resistant GNRs Prevalence of isolates of multidrug-resistant gram-negative bacilli recovered within the first 48 h after admission to the hospital, by species. Only 1 isolate per patient per year was included in the study. Pop-Vicas, Clin Inf Dis 40:1794 2005 (MGH)
Results of intensive care unit surveillance revealing rates of antimicrobial resistance to third-generation cephalosporins among Klebsiella pneumoniae isolates (which includes isolates that were either intermediately susceptible or resistant) and Escherichia coli isolates—National Nosocomial Infections Surveillance system, 1986–2003. Gaynes R CID 2005 (CDC)
INCIDENCE RATES OF MULTIDRUG-RESISTANT BACTERIA PER 100 ADMISSIONS: STAPHYLOCOCCUS AUREUS (LINE WITH BLACK DIAMONDS), PSEUDOMONAS AERUGINOSA (LINE WITH WHITE DIAMONDS), ENTEROBACTERIACEAE (LINE WITH BLACK BOXES), AND ACINETOBACTER BAUMANNII (LINE WITH WHITE BOXES). Lepelletier D ICHE 2004--Nantes
Resistant GNBThe Problem • High mortality • Narrowing therapeutic options • Down to carbapenems, polymixin B
New antibacterial agents approved in the United States, 1983–2002, per 5-year period. Spellberg B et al. Clin Inf Dis 2004
Resistant GNBThe Problem • Hard to detect: may be in your building for months/years before you get worried • Not sexy; no media exposure • How to compete with alarms about MRSA?
Resistant GNB • Organisms of concern: • Pseudomonas aeruginosa • Acinetobacter baumannii • Enterobacteriaceae: • Klebsiella pneumoniae • Enterobacter spp. (esp cloacae) • E. coli • Serratia marcescens
Sites of infection with extended-spectrum β-lactamase–producing Escherichia coli and Klebsiella species: 187 patients at HUP, over 5 y Hyle EP Arch Int Med 2005 (HUP)
Resistant GNBClinical Significance • High mortality, especially with pneumonia or BSIs • Clear effect of delay in appropriate therapy on survival • 40-100% mortality when treating apparently susceptible deep infections with Klebsiella with cephalosporins
Delay in initial antimicrobial therapy and mortality. Hyle EP Arch Int Med 2005 (HUP)
Resistant GNBClinical Significance • NNIS data • 20% of ICU Klebsiella isolates are resistant to 30 cephalosporins • 30% of ICU Enterobacter isolates similar • 6% of E. coli isolates similar • (Netherlands: <1% of Klebsiella with ESBLs!)
Resistant GNBEpidemiology • Risks for acquisition: No surprises • Current and previous abx Tx • Older patient (>60 y) • ICU stay; prolonged ICU stay • IV catheters; tubes of every kind • NH/LTCF denizen (1/2 colonized with ESBLs!) • H2 receptor blockers (Zantac et al) • Chronic liver/renal disease
Safdar N, Maki DG, Ann Int Med 2002;136:834
Resistant GNBEpidemiology • Risk of deep infection >> if previously colonized (40 fold) • 15% of colonized patients go on to invasive infection • Rare “community-acquired”
Resistant GNBEpidemiology: when/how acquired? • Horizontal transfer vs endogenous source • Unlike MRSA, VRE---overwhelmingly horizontal transfer • Endogenous: • Enterobacteriaceae seldom spontaneously resistant; Pseudomonas not cultured from normal individuals (Acinetobacter +/-) • But resistance in same clone emerges commonly under antibiotic pressure
Resistant GNBEpidemiology: when/how acquired? • Clearly some horizontal transfer though • How? • 5% (<< MRSA) of area around bedside of colonized patients are colonized with resistant GNBs---but they’re there– environmental reservoir • (Clearly documented point source outbreaks) • Large (undetermined) percentage of colonization occurs through HCWs hands (esp Klebsiella and Acinetobacter)
PERCENTAGE OF HAND IMPRINT CULTURES YIELDING PATHOGENS AFTER CONTACT WITH ENVIRONMENTAL SURFACES NEAR PATIENTS IN OCCUPIED PATIENT ROOMS OR IN ROOMS THAT HAD BEEN CLEANED AFTER PATIENT DISCHARGE. Bhalla A ICHE 2004 (Cleveland)
Distribution of infant and nurse clones identified as unique strains, strains shared between nurses and infants, and strains shared between nurses or among infants. Waters V, Clin Inf Dis 2004 (Columbia)
Resistant GNBBasis of Resistance • Pseudomonas aeruginosa, Acinetobacter spp. Intrinsically resistant through multiple mechanisms: • β-lactamases—many possible • Aminoglycoside modifying enzymes • Porin mutations, with abx exclusion • Efflux pumps up and running • Topoisomerases for FQs
Resistant GNBBasis of Resistance • Enterobacteriaceae: β-lactamases rising • 1960’s—routine enzymes (TEM 1, SHV 1): ampicillin, Keflex resistant • 1980’s—mutations; “extended spectrum”—DNA encoded on plasmids, jump to other GNBs easily • Active against 30 cephalosporins, aztreonam • Not active (stay susceptible) against cefoxitin, cefotetan, and β-lactamase inhibitors (Zosyn, Augmentin, Unasyn) • Currently >100 ESBLs recognized
Resistant GNBBasis of Resistance: Example Klebsiella pneumoniae, old TEM 1: Amp R Keflex R Cefoxitin S Cefotaxime/ceftriaxone S Ceftazidime S Cefipime S Zosyn S Cipro S Aminoglycoside S Bactrim S
Resistant GNBBasis of Resistance: Example Klebsiella pneumoniae, old TEM 1; new ESBL: Amp R R Keflex R R Cefoxitin S S Cefotaxime/ceftriaxone S R Ceftazidime S R Cefipime S (S) Zosyn S S Cipro S (S) Aminoglycoside S (S) Bactrim S (S)
Resistant GNBBasis of Resistance • Amp C β–lactamases: newer, broader R • Chromosomal: don’t jump so much • Mostly on Enterobacters; rare Kleb • Do cause R to cefoxitin, and β–lactamase inhibitor combinations
Resistant GNBBasis of Resistance: Example Klebsiella pneumoniae, old TEM 1; new ESBL; Amp-C Amp R R R Keflex R R R Cefoxitin S S R Cefotaxime/ceftriaxone S R R Ceftazidime S R R Cefipime S (S) (S) Zosyn S S R Cipro S (S) (S) Aminoglycoside S (S) (S) Bactrim S (S) (S)
Resistant GNBBasis of Resistance • ESBLs and Amp-C β–lactamases are inoculum dependent • Usual tests are at low inoculum; may look S • In vivo, high loads of bugs common; clinical failures of the “S” abx is common • Requires special testing techniques • If not performed, ESBL/Amp-C bugs may look S but your patients are dying • CLSI recommends specific testing; if ESBL or Amp C are found, trust NO and treat with NO β-lactam except carbapenem (imipenem, meropenem, ertapenem)
Resistant GNBDeceptive Susceptibility Testing: ESBLs May Look Sensitive Klebsiella pneumoniae Amp R Keflex R Cefoxitin S Cefotaxime/ceftriaxone S Ceftazidime (S) Cefipime S Zosyn S Cipro S Aminoglycoside S Bactrim S
Resistant GNBDeceptive Susceptibility Testing: Amp-C’s May Look Sensitive Early On Enterobacter spp. Amp-C early Amp C 3-10 d later Amp R R Keflex R R Cefoxitin S R Cefotaxime/ceftriaxone S R Ceftazidime S R Cefipime S (S) Zosyn S R Cipro (S) (S) Aminoglycoside (S) (S) Bactrim (S) (S)
Double-disk susceptibility test for ESBLs, this time in Enterobacter cloacae. AMC (center) = clavulanic acid; FEP = cefepime; CAZ = ceftazidime; CXT = cefotaxime; CRO = ceftriaxone
Resistant GNBTreatment • Must pick adequate coverage immediately (reviewed already). • Greater survival differences in under-treated resistant GNBs than even under-treated MRSA • Patients at risk should receive broader coverage • Carbapenems; +/- double GNB coverage
Rahal et al Clin Inf Dis 2002;34:501 “Squeezing the balloon”. Evolution and control of antibiotic resistance among gram-negative bacilli at New York Hospital Queens. ICU, intensive care unit.
Resistant GNBInfection Control Issues • Prevention of transmission of resistant Staphylococcus aureus and Enterococcus specifically addressed in 2003 SHEA guideline* • Call for active surveillance cultures, based on • Recognition that colonization precedes infection • Response with barrier precautions works to reduce clinical infections • Response if wait till clinical cultures return positive is less impressive (vs no help) * Muto CA ICHE 2003;24:362
Resistant GNBInfection Control Issues • HICPAC guidelines address all MDROs* Call for measured response: Active surveillance (rectal cultures in case of ESBLs) if institution “has a problem” • Otherwise, adjust level of surveillance/recognition to overall need, or focus on geographic areas in house (e.g., ICUs) • Decisions made on basis of your institution’s amount of problem, resources, administration’s interest† * Siegel et al www.cdc.gov/ncidod/dhqp/pdf/ar/mdroGuideline2006.pdf † Discussion at Jackson M et al AJIC 2004;32:504
Resistant GNBInfection Control Issues • Other components of infection control: • Antibiotic stewardship program* • Probably as or more important here than for other MDRO’s • Carbapenems for empirical therapy; avoid ceftazidime; avoid 30 cephalosporins in general (Zosyn maybe helfpul) • Contact precautions*: interrupt environmental risk • Determine clonality if available (also, ? Point source?) * Good evidence intervention works
Resistant GNBInfection Control Issues • Hand hygiene* • Cohorting patients*, cohorting staff* • Good staffing ratios* * Good evidence intervention works
Resistant GNBInfection Control Issues • Cautions: • Contact precaution data is not usually in isolation • Active surveillance costs: • Money • Time • Effort


![GRAM NEGATIVE BACILLI- MICRO {ST1]](https://cdn1.slideserve.com/2240310/gram-negative-bacilli-micro-st1-dt.jpg)