Download
1 / 44
450 likes | 747 Views
Maternal, Infant, and Early Childhood Home Visiting Program (MIECHV) Supplemental Information Request #2 ( SIR #2) Virginia Updated State Plan Regional Meetings March 21-30, 2010. Maternal, Infant, and Early Child Home Visiting. Purposes:

E N D
Maternal, Infant, and Early Childhood Home Visiting Program(MIECHV) Supplemental Information Request #2 (SIR #2) Virginia Updated State Plan Regional Meetings March 21-30, 2010
Maternal, Infant, and Early Child Home Visiting • Purposes: • to strengthen and improve the programs and activities carried out under Title V of the Social Security Act; • to improve coordination of services for at-risk communities; and • to identify and provide comprehensive services to improve outcomes for families who reside in at-risk communities
Application Process • Step 1: July 2010 State applications • Step 2: September 20, 2010 SIR #1 • Statewide Needs Assessment • Step 3: Supplemental Information Request #2 • Updated State Plan • Due June 8, 2011
Updated State Plan • Final designation of at-risk communities to be targeted by State HV Program • Detailed needs and resources assessment for communities • Plan for coordination among existing programs/resources • Assessment of local and State capacity to integrate the proposed home visiting services into an early childhood system • A list of “at-risk” communities not selected for implementation in FY 2010
Updated State Plan • Goals and Objectives of Updated Plan • Strategies for Integrating Updated State Plan into other early childhood programs and systems • Logic model for State HV Program
Selection of Model • Selection of the model(s) should be in response to the needs of the targeted at-risk communities • Select a model(s) that meets criteria for evidence of effectiveness • Propose another model not reviewed by HomVEE study • Request reconsideration of an already-reviewed model • Propose use of up to 25% of funds for a promising approach
Evidence-based (EB) Models (2/08/2011)http://www.acf.hhs.gov/programs/opre/homvee • Early Head Start- Home-based Option Only • Family Check-Up • Healthy Families America • Healthy Steps • Home instruction Program for Preschool Youngsters (HIPPY) • Nurse Family Partnerships • Parents as Teachers
State Selection of Model • Within 45 days, States must secure approval by developer(s) to implement model(s) as proposed, including any acceptable adaptations • For the MIECHV program, an acceptable adaptation is one determined by the developer not to alter the core components related to program impacts
Implementation • States must: • Describe how the model(s) meets need of each community • Describe State’s current and prior experience implementing model(s) • Submit a plan for ensuring implementation with fidelity • Discuss anticipated challenges to implementation
Implementation • State must: • Submit a plan for implementation of State HV Program and for ongoing monitoring of the quality of implementation at the community, agency, and participant level • Submit required assurances • Must agree to the Maintenance of Effort
Maintenance of Effort (MOE) States must : Maintain the level of State General Funds As of March 23, 2010
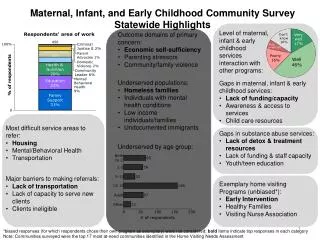
Benchmarks • Maternal and Newborn Health • Child injuries; child abuse, neglect, or maltreatment • School readiness and achievement • Crime or domestic violence • Family economic self-sufficiency • Coordination and Linkages
Benchmarks • State must : • Collect data on all 6 benchmark areas • Collect data for all listed elements under each benchmark area • Show improvement in at least half of the elements under each benchmark area • Develop a continuous quality improvement plan • Report to HHS on benchmark progress at the 3-and 5-year points
State Home Visiting Plan • A description of the administrative structure in place to support the program • A description of staffing and administration • A description of efforts to coordinate the program with other State early childhood plans
Continuous Quality Improvement • CQI is an approach utilizing regular data collection and the application of changes that may lead to performance improvements • The State must discuss a plan for CQI for their State HV Program • Technical assistance will be provided as needed on CQI strategies
Technical Assistance • HHS intends to provide TA and training to States throughout the grant application process and implementation phase of the MIECHV Program • States should provide a description of anticipated TA needs in the Updated State Plan • State level • Local communities
Memorandum of Concurrence Signed by: • Director of the State’s Title V agency • Director of the State’s agency for Title II of the Child Abuse Prevention and Treatment Act (CAPTA) • Director of the State’s child welfare agency (Title IV-E and IV-B), if this agency is not also administering Title II of CAPTA • Director of the State’s Single State Agency for Substance Abuse Services • State’s Child Care and Development Fund (CCDF) Administrator • Director of the State’s Head Start State Collaboration Office and
Memorandum of Concordance(continued) • State Advisory Council on Early Childhood Education and Care authorized by 642B(b)(1)(A)(i) of the Head Start Act • The State’s Individuals with Disabilities Education Act (IDEA) Part C and Part B Section 619 lead agency(ies) • State Elementary and Secondary Education Act Title I or State pre-kindergarten program and • State Medicaid/Children’s Health Insurance program (or the person responsible for Medicaid Early Periodic Screening, Diagnosis, and Treatment (EPSDT) Program).
Additional Potential State Partners • State Domestic Violence Coalition • State identified agency charged with crime reduction • State Temporary Assistance for Needy Families agency • State’s Supplemental Nutrition Assistance Program agency • State Injury Prevention and Control (Public Health Injury Surveillance and Prevention) program
Federal Review • Justification of targeted communities at risk • How the model(s) addresses specific community needs • Plan for meeting benchmarks and collecting data • Overall feasibility of plan • Level of commitment and concurrence among required partners
Virginia Needs Assessment • Insufficient staff to provide for the unmet need for HV • Services for fathers • Services for teen parents • Services for diverse cultural populations • Unavailable mental health and substance use treatment resources for parents • Inadequate domestic violence prevention and treatment • Insufficient parent support in crisis situations, especially to prevent abuse/neglect • Increased need for education/training for parents so that they can be self-sufficient • Addition: Early and appropriate referral to Early Intervention
Virginia Plan • Parallel the Federal Requirements • Provide Technical Assistance to all 38 “at-risk” communities • Integrate Home Visiting Services into the Early Childhood system with staff training, data collection, evaluation • Require local Data Collection in the state project system • Develop Continuous Quality Improvement Plan (CQI)
Virginia Plan • Increase Quality, Effectiveness and Availability at the State and Local level • Increase services by Evidence-based (EB) Home Visiting Models in local communities • Show Improvements in the Lives of Vulnerable Families and Their Children as measured by Progress toward the Benchmark Goals within 3 to 5 years
State Application Process • Eligible Applicants: • 38 “at risk” Communities or • a zip code area or adjacent zip code areas which meet the same qualifications as the 38 “at risk” communities • Requirements: Still being reviewed • Due date: TBA
Accomack County Bristol City Campbell County Charlotte County Cumberland County Danville City Emporia City Essex County Fredericksburg City Gloucester County Greensville County Halifax County Hampton City Henry County Hopewell City Lancaster County Lunenburg County Lynchburg City Montgomery County Newport News City Norfolk City Northampton County Nottoway County Orange County Patrick County Petersburg City Portsmouth City Radford City Richmond City Smyth County Southhampton County Staunton City Suffolk City Sussex County Warren County Waynesboro City Williamsburg City Winchester City Virginia “at-risk” Communities
First Steps for Local Application • Meet with all local home visiting programs • Invite early childhood partners • Meet with the local Early Childhood Coalition (Smart Beginnings Coalition or others)
Identify Community Home Visiting Needs Use existing needs assessments to begin • City/County Development Plan • Local Dept of Social Services • Local Health Department (MAPP) • Local Community Service Board • Local School System data or plans • Head Start Needs Assessment • Juvenile Justice Prevention Plan • Early Intervention Office • Early childhood Interagency Group • Housing Department • Boys and Girls Club; etc
Ask parents & other consumers • Parents/Families • Parents with children in Head Start and other early child education settings • WIC participants • New Parent Classes/Childbirth Classes • Community Advocacy Groups • Professionals • Local Obstetricians and Pediatricians; Providers in Medical Homes; Community health care centers • Teachers at early childhood centers • Business leaders • Hospitals
Identify Gaps in Local Home Visiting Services(children ages 0-5 years old; families) • Age Group • Risk factors • Neighborhood • Cultural factors
Identify Resources • Commitment to Improving Services • History of supporting Families • Experienced Staff • Successful Organizations • Communication Networks • Interagency Collaborative History • Relationships with other “at-risk” Localities • Community Opportunities
Identify a Target Population • Priority to Vulnerable Families • Low income • A Pregnant women who is less than 21 years old • A History of Child Abuse and Neglect • A History of Substance Abuse or in need of treatment • A History of using Tobacco products in the Home • Low achievement, or have children with, Low Achievement • Those with children with Developmental Delays • Family members serving in the Armed Forces or on multiple deployments outside of the United State.
Selection of an Evidence-based Model • Identify the Community Goals • Review Community Needs • Consider Community Gaps • Identify Target Population • Commit Community Resources
In Selecting the Model(s) • Pay particular attention to the Target Population identified for each model • Review the Evidence-based Model report by Mathematica Policy Research • Review the HomVee website
Selection of the Model(s) • There is not one “right” selection. • A review of the Needs, Gaps, Resources, Community Experience and Target Populations could lead to the choice to expand an existing evidence-based program model or to add a new program model to the community continuum in order to best serve vulnerable families. • Consider where the community is interested in making an effort. • Make a clear logical explanation of the choice.
Local Community Applicant • Each community is likely to be asked to demonstrate: • Evidence of Efficiency and Effectiveness in Plan • Cost per Child / per Family • Evidence of Collaboration • Evidence of Experience and Solid Performance in providing HV services • Consumer/Community Interest/input/buy-in • Evidence of Commitment to Improvement on Benchmarks • Local Opportunities for Broader Partnership
Home Visiting Consortium • Ashley Barton - BabyCare, Department of Medical Assistance Services • Mary Mitchell - Medicaid Managed Care, DMAS • Johanna Schuchert - Healthy Families • Ann Childress – Dept of Social Services (DSS) • Lisa Specter-Dunaway - CHIP of Virginia • Linda Foster - Virginia Healthy Start Initiative, Dept of Health (VDH) • Wenda Singer - Head Start/Early Head Start Collaborative, DSS • Phyllis Mondak - Special Education/Part B, Dept. of Education • Mary Ann Discenza – Early Intervention/ Part C, Depart of Behavioral Health and Developmental Services (DBHDS) • Martha Kurgans – Project Link, DBHDS • Catherine Bodkin - Resource Mothers, BabyCare Liaison, (VDH)
Useful Websites • www.homevisitingva.com • www.homvee.acf.hhs.gov • www.mdrc.org/project_12_104.html • www.mchcom.com
www.homevisitingva.comSee “Announcements” or “Resources/Virginia documents”
www.homevisitingva.comAnnouncements and Documents are posted here. Contact: Any Member of the Virginia Home Visiting Consortium or Catherine Bodkin, LCSW, Chair of HVC MIECHV Project Director Virginia Department of Health Catherine.bodkin@vdh.virginia.gov 804-864-7768
QUESTIONS? Thank you for participating today.