Download
1 / 36
360 likes | 575 Views
Chapter 10 Inflammation. Inflammation is a process carried out in response to either physical or immunological tissue insult. It consists of a destructive process to remove the inflammatory trigger and damaged tissue, followed by repair and replacement.

E N D
Chapter 10 Inflammation Inflammation is a process carried out in response to either physical or immunological tissue insult. It consists of a destructive process to remove the inflammatory trigger and damaged tissue, followed by repair and replacement. The main actors in the destructive phase are neutrophils and macrophages. Inflammation is signaled by heat, pain, redness, and swelling (calor, dolor, rubor, tumor). Inflammatory conditions are named with the suffix itis.
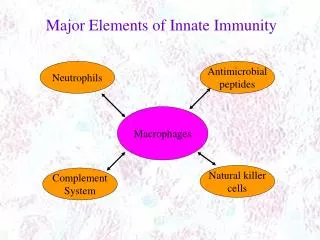
Macrophages are highly complex cells engaged in normal tissue maintenance and turnover. Among their varied functions, they are sentinels against infection, both through the use of receptors for common molecules carried by pathogens, and through opsonization. Macrophages exist in various levels of activation, wherein they become more aggressive at destroying macromolecules, and sending distress signals to recruit other components of the inflammatory response. The most aggressively activated macrophages are derived from blood monocytes in response to inflammatory signals. These are called “infiltrating macrophages”.
Names of Macrophages According to Tissue Locations Location Connective tissue Serous cavity Liver Bone tissue Lung Nervous system Spleen Skin Inflamed tissue Name Histiocyte Peritoneal macrophage Kupffer cell Osteoclast Alveolar macrophage (dust cell) Microglial cell Sinusoidal lining cell Langerhans cell Infiltrating macrophage
Macrophage activation: Toll-like receptors (TLR1-10) & C-type lectin receptors: Moieties found in cell walls of Gram positive and Gram negative bacteria, Mycobacteria, Trypanosomes, Treponema, Neisseria; bacterial flagellin; viral glycoproteins; dsRNA; virus single stranded RNA; unmethylated CpG DNA; malarial pigment haemozoin; Toxoplasma gondi profilin-like protein; HIVgp120; fungus b-glucans; zymosan. T lymphocyte signaling Interferon g Opsonization: Immune complexes with IgG, IgA, activated complement on bacterial cell wall.
Homing lymphocyte selectin binds endothelial addressin cellular integrins bind endothelial ICAM/VCAM
Cells involved in inflammatory response Neutrophils Monocytes -> Infiltrating Macrophages T lymphocytes Resolution phase: Epithelial cells Fibroblasts
Leukocytes and % of Each Type in Blood Nongranular Monocytes Lymphocytes Granular Neutrophils Eosinophils Basophils % 59.0 2.7 0.3 % 4.0 34.0
Some cytokines involved in inflammatory responses IL1 Macrophage distress signal; recruits and activates CD4 and CD8 T cells; systematically causes fever. Drives TH1 response. INFg, IL2 IL4,5 Drives TH2 response; suppresses TH1 response. Deactivate macrophages; stimulate resolution; promote matrix synthesis; switch B cells from IgG to IgA. TGFb IL3 Stimulates production of more blood cells. IL8 Chemotactic factor for neutrophils. INFa,b Shuts down translation; initiates virus-resistant state.
Mediators of inflammatory responses Histamine Kinins Serotonin Kinins are produced from kininogens during the coagulation cascade. Serotonin is released from platelets during platelet activation.
Neutrophil/ macrophage interaction Activated neutrophils secrete oxygen radicals, antimicrobial peptides, lysosomal granule contents, and signals to attract monocytes. Monocytes differentiate to macrophages which will remove dead neutrophils and their secreted products.
Kinin (bradykinin) receptors Acute inflammation Chronic inflammation B2 receptor B1 receptor Constitutively expressed Induced by chronic stimulation Rapidly desensitized Not desensitized
When phagocytes fail to remove the inflammatory trigger: Purulent exudate (pus) formation in an abscess – typically means that a bacterial pathogen is resisting killing by macrophages. Fibrosis – formation of abnormal scar tissue because repair cells can not properly access the still-inflamed area. Chronic inflammation – a long term state of inflammation in which there will be loss of tissue.
Periodontal probe used to measure depth of periodontal pocket
Steps and inhibitors of hemostasis 1. Vascular spasm 2. Platelet plugging aspirin (acetylsalicylic acid), plavix (colpidogrel) 3. Coagulation coumadin (warfarin), dicoumerol (active form of coumarin)
Vascular Spasm Contraction of smooth muscle cells surrounding the injured vessel. Upstream constriction reduces blood loss. Can last 30 minutes. Signaled by: Thromboxane A2 Thrombin
Platelet activation Receptors: Glycoprotein Ib/V/IX --> von Willebrand Factor Glycoprotein Ia --> collagen Glycoprotein VI --> collagen Glycoprotein IIb/IIIa --> fibronectin, other platelets Signals: Thromboxane A2 (COX pathway) [inhibited by aspirin] (Other N.S.A.I.D.s inhibit COX, but are reversible inhibitors). ADP [inhibited by plavix]
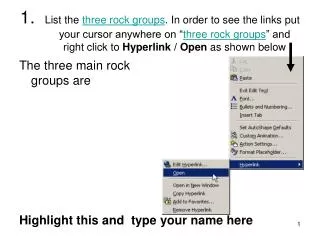
True or False? http://biochem.uthscsa.edu/hardies-bin/survey.pl The glycoproteins of this kind are generically called “adhesion proteins” Three of the proteins are of a class called “integrins”. Integrins exhibit “inside out” signaling. That means: a) When activated, the cell turns inside out. b) When it binds its ligand, a signal is passed into the cell. c) When the cell is activated, it shifts the integrin from an inactive to an active binding conformation. d) They cause platelets to become “sticky”.
True or False? http://biochem.uthscsa.edu/hardies-bin/survey.pl NSAIDs (non steroidal anti inflammatory drugs) include: • aspirin • ibuprofin • tylenol • naproxin • prednisone
carboxylase inactive factor gamma carboxylated factor vitamin K vitamin K epoxide O vitamin K epoxide reductase dicoumerol coumadin (warfarin)
Coagulation Complexes Kallikrein kinin XIIa preKallikrein XII HMW kininogen neg. surface VIIa X X IXa Ca+2 Ca+2 Xa VIIIa Ca+2 Ca+2 TF platelet surface tissue cell Xa II IIa Ca+2 Ca+2 Va platelet surface
Coagulation Pathways collagen fibers PTT + + kininogen Inflammation kinin hemophilia B + Coumadin PT/INR hemophilia A vWF + Coumadin + Coumadin Tissue cell Coumadin + + platelets (platelet count; platelet function assay) ristocetin +vWF aggregation aspirinplavix
True or False? http://biochem.uthscsa.edu/hardies-bin/survey.pl • The lab test for coagulation integrity in a patient taking coumadin is PTT. • von Willebrand Disease can look like a mild factor VIII deficiency. • A lab test for adequate compensation for classic hemophilia is INR. • A specific test for von Willebrand Disease is the ristocetin agglutination assay.
Regulation of coagulation heparin: chopped up glycosaminoglycan released from mast cells, or administered clinically. Stimulates antithrombin III, which inhibits factors IIa, IXa, Xa, XIa, and XIIa. Reversed by protamine sulfate. heparan sulfate: on surface of endothelial cells acts like heparin. thrombomodulin: on surface of endothelial cells; activates Protein C & S; Protein C cleaves and inactivates factors VIIIa and Va. prostaglandin I2 (PGI2): secreted by endothelial cells inhibits platelet activation.
Fibrinogen Thrombin removes N ter. propeptides fibrin half staggered array
Fibronectin crosslinked to fibrin
Fibrinolysis plasminogen plasmin tissue plasminogen activator
Causes of abnormal bleeding Genetic Diseases affecting platelets leukemia, AIDS hemophilia. A (F-VIII), B (F-IX). X-linked Diseases affecting the liver von Willebrand Disease cirrhosis up to 1%, men or women Vascular fragility Drugs vitamin C deficiency, connective tissue disorders coumadin, plavix, aspirin, chemotherapy, alcohol, broad spectrum antibiotics
Laboratory Tests Platelet count Prothrombin time (PT/INR) plasma from patient plus thromboplastin (contains triggers of extrinsic pathway) Measures 3 Vit K dependent factors. VII has shortest half life of vitamin K-dependent factors. Time to clot normalized by normal controls and adjusted for the potency of the thromboplastin is called INR (0.8 – 1.2 is normal). Partial thromboplastin time (PTT) plasma from patient plus thromboplastin (without TF) plus trigger of intrinsic pathway.
Functions of the clot Stop bleeding Seal against infection Scaffold for epithelial cells, and for deposition of granulation tissue