Download
1 / 89
910 likes | 1.71k Views
Hemochromatosis. BCSLS Telehealth Presentation October 19, 2006 Gillian Lockitch, MBChB, MD, FRCPC. OBJECTIVES. Review iron absorption and transport Describe types of hemochromatosis Hemochromatosis and the laboratory Suspicion Investigation Diagnosis. Iron Absorption and Transport.

E N D
Hemochromatosis BCSLS Telehealth Presentation October 19, 2006 Gillian Lockitch, MBChB, MD, FRCPC
OBJECTIVES • Review iron absorption and transport • Describe types of hemochromatosis • Hemochromatosis and the laboratory • Suspicion • Investigation • Diagnosis
Fe+3 Fe+2 Fe+3 Fe+2 Fe Fe Transferrin Fe Fe Villus enterocyte Fe2+ Fe+2 Fe+3 Ferritin Macrophage Ceruloplasmin Bone Marrow Liver
3 - 4 g 1 – 2 mg 1- 2 mg Total body iron Daily iron absorption Daily iron loss OTHER Menstrual (monthly) pregnancy (total) Normal Iron metabolism Male Female • 2 - 3 g • 1 – 2 mg • 1- 2 mg OTHER • 20 - 40 mg • 600 - 900 mg
Fe+3 Fe+2 Ferritin 1 – 2 mg /d 1 – 2 mg /d Macrophage Fe Fe Fe2+ Villus enterocyte 20 mg / d Liver Menstruation 20 – 40 mg /m Bone Marrow
Fe+3 Fe+2 Ferritin 7 – 8 mg /d 1 – 2 mg /d Macrophage Fe Fe Fe2+ Villus enterocyte 20 mg / d Liver Menstruation 20 – 40 mg /m Bone Marrow
Iron transport and absorption proteins • Transferrin • Ferritin • Transferrinreceptor • Ceruloplasmin
Non-heme iron absorption process • Reduction of ferric to ferrous iron • Transport across brush border • Sequestration in enterocyte • Basal transport from cell • Oxidation to ferric form • Transport by transferrin • Uptake by transferrin receptors • Utilisation or storage
Fe 2+ Fe 2+ Fe 2+ Fe 3+ Fe 3+ Fe 2+ Reduction of ferric to ferrous iron Ferric reductase Transport across brush border Divalent metal transporter 1 (DMT1) Ferric reductase DMT1 Sequestration in enterocyte Ferritin Basal transport from cell Ferroportin Hephaestin Ferroportin (IReg1) Oxidation to ferric form Hephaestin Ceruloplasmin
Iron regulates the synthesis of its own key transport and storage proteins Iron responsive elements (IREs) Iron responsive element binding proteins (IRPs)
DNA transcription Messenger RNA translation Protein
Iron Responsive Elements (IREs) Low intracellular iron: IRP binds and prevents mRNA translation Low intracellular iron: IRP binds and stabilizes mRNA mRNA transcript IRE IRE 5` 3` Untranslated regions IRP1 and IRP2 - Binding Proteins
Proteins with 5’ or 3’ IREs • 5’ - low iron decreases synthesis • Ferritin • Ferroportin • Erythroid heme aminolevulinic acid synthase • 3’ - low iron prevents mRNA degradation • Transferrin receptor 1 • DMT1 (divalent metal transporter)
Ferritin Low intracellular iron content High intracellular iron content IRP bound mRNA not translated ferritin low IRP not bound mRNA translated ferritin synthesized mRNA transcript 5`
DMT1 Control of synthesis Low intracellular iron content IREs mRNA transcript 3` RTD IRPs bound - mRNA stabilized ongoing TfR synthesis when IRP is bound to the IRE binding of ribonuclease to rapid turnover domain (RTD) is blocked
Fe 2+ Fe 2+ Fe 2+ Fe 3+ Fe 3+ Fe 2+ Ferric reductase DMT1 hephaestin ferroportin (IReg1)
modulation of iron absorption by intestinal villi Mature enterocytes Crypt cell
Villus Enterocyte DMT1 mRNA Fe 2+ Fe 3+ Crypt Cell Fe 3+ Fe 2+ Low iron state
Fe+3 Fe+2 Fe+3 CP Fe+2 DMT1 Fe Ferric reductase Fe Fe2+ Fe2+ FPN1 Ferritin Villus enterocyte Hypoxia _ _ Erythropoietin Macrophage _ mRNA(DMT1) 5’ 3’ + Hemojuvelin IRP IRP-Fe Crypt cell Hepcidin TfR2 FPN1 Fe2+ + _ _ Liver TNF-α Fe Fe + Holotransferrin Inflammatory Stimuli (IL-6; Lipopolysaccharide)
Proteins of iron transport • Transferrin / Ferritin • Transferrin receptors: TfR1, TfR2 • Ceruloplasmin / Hephaestin • Divalent Metal Transporter 1 • Ferroportin • IRP1 and IRP2 (cytosolic mRNA binding) • HFE protein • ß-2 microglobulin • DCyt B (ferric reductase) • Hepcidin • Hemojuvelin
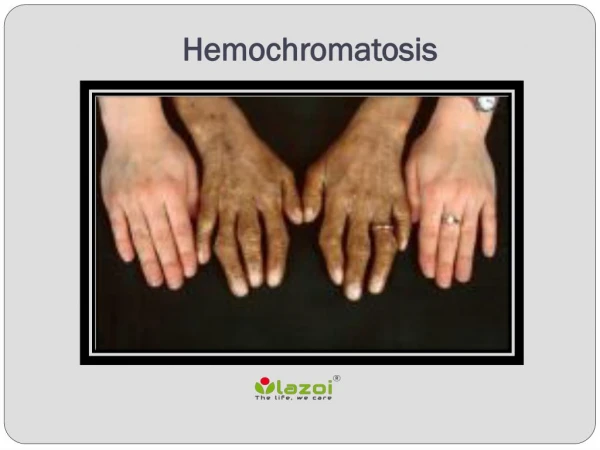
Classical Hemochromatosis • First description 1865 • inherited disorder 1935 • autosomal recessive disorder of excess iron deposits in parenchymal tissues causing organ damage and dysfunction • Affects liver, pancreas, heart, joints, pituitary, skin – “bronze diabetes” • Considered rare disease of elderly men
Hemochromatosis by 1996 • Syndrome preventable if iron overload diagnosed and treated early. • Treatment simple: - phlebotomy • Recognition – high transferrin saturation and ferritin • Studies of blood donors suggested that 1:200 to 1:400 people have biochemical iron overload • Much more common than originally thought • 1 in 200 in NW European populations
HFE B C E A HLA genes C282Y mutation in HFE gene In late 1996 an HLA linked gene on chromosome 6 p 21.3 was found to be associated with hemochromatosis patients of North West European origin
HFE mutations in Caucasians A single mutation, C282Ywas shown to be associated with hemochromatosis in around 80% of patients of NW European origin
Genetics: Homozygosity for C282Y very common in NW Europeans (1:200) • Biochemistry: Most homozygotes will slowly accumulate iron leading to high ferritin and transferrin saturation > 55% • Clinical: Disease penetrance very variable from early symptoms and severe disease to no symptoms – genetic diagnosis very common – but the disease syndrome much less so
Study of 26,000 genotyped subjects from San Diego Kaiser Permanente clinic • (Beutler: Lancet 2002;211-128) • 152 homozygotes – only 1 with clinical syndrome – penetrance 1% • Fatigue, arthralgias, impotence, arrhythmias no more prevalent than in non-C282Y homozygotes • Only significant difference was 5-10% had abnormal liver function tests
Family - HFE.1. C282Y
Adult-onset Hemochromatosisdue to TfR2(transferrin receptor 2)mutations
Referred for HFE testing • 35 year old man • severe iron overload • ferritin 34,000 • saturation 0.90 • results: C282Y wt / wt H63D wt/ mut TRF2 Study: Mattman, Vatcher, Ralston Huntsman, Lockitch, Langlois et al
E60X M172K Y250X Q690P Homozygous 5’ 3’ Heterozygous A75V I238M* A376D N402K R752H X3 X4 Previously described homozygous mutations Novel homozygous mutation Novel heterozygous sequence variation Mattman et al. Blood: 2002; 100; 1075-7 * Previously described sequence variant
Q690P 1 2 I 1 2 3-9 10 11 II 7 7 8 9 10-11 1-5 6 III 5 2 67 Ferritin 45 Sat 2 3 1 4 IV 36 35 30 25 Age Ferritin saturation 39 30 35 95 34000 90 234 77
Patient Genotype ccg homozygote pro/pro cag/ccg heterozygote gln/pro cag homozygote gln/gln ccg homozygote pro/pro ccg homozygote pro/pro IV-2 III-8 IV-I IV-3 IV-4
Juvenile Hemochromatosis Type 2.A Hemojuvelin Type 2.B Hepcidin
Juvenile Hemochromatosis • autosomal recessive disorder • affects male and female equally • Usually presents between 10 and 30 years • severe iron overload, organ failure and high mortality rate • hypogonadism and cardiomyopathy are prominent features • Also cirrhosis, diabetes, arthopathy
Juvenile Hemochromatosis • Of the first 16 reported cases – diagnosed at 4 – 19 years • 11 died within 2 years of diagnosis • Congestive heart failure • Severe cirrhosis and liver failure
Family JH.1 1987 • A 7 year old girl saw her GP because her teacher thought she looked very pale. • Her blood count parameters were normal but her ferritin was 339 and transferrin saturation 0.94 • Her younger siblings also had high ferritin and saturation
Family JH.1 Sat 0.33ferritin 95 Sat 0.26ferritin 81 Age 7Sat 0.94 ferritin 339 Age 6Sat 0.90 ferritin 146 Age 4Sat 0.59 ferritin 187
Family JH.1 Liver iron content 7 yr 6 yr 4 yrN hepatic iron 8254 6582 4679 < 290 HII 21.1 19.6 20.9 1 2 years later after regular phlebotomy hepatic iron 1588 795 2141 HII3.16 1.58 7.67 ferritin 15 21 35 sat 0.6 0.8 0.9
Sat0.33ferritin 95 Sat0.26ferritin 81 Age 7 Sat 0.94 ferritin 339 Age 6 Sat 0.90 ferritin 146 Age 4 Sat 0.59 ferritin 187 Family JH.1 1997 HFE testing C282Y H63D
Sat 0.33ferritin 95 Sat 0.26ferritin 81 Age 7 Sat 0.94 ferritin 339 Age 6 Sat 0.90 ferritin 146 Age 4 Sat 0.59 ferritin 187 Family JH.1 2004 HFE2 (HJV) hemojuvelin Testing I222N G320V
Eleven years post diagnosis • Treated rigorously with phlebotomies ever since diagnosis • Seen at 18, 17 and 14 years respectively • No evidence of cardiac, hepatic or endocrine dysfunction
Family JH.2 • A 19 year old boy presented in severe cardiomyopathic heart failure. He was a candidate for heart transplantation • Transferrin saturation was 100% and ferritin 1403 • Following intensive phlebotomy therapy cardiac function improved dramatically and transplant was avoided.
Family JH.2 C282Y 1997 HFE testing Sat 0.21 ferritin 26 Sat 0.26 ferritin 90 Age 19 Sat 1.00 ferritin 1403 Age 19 Sat 0.24 ferritin 30 Age 21 Sat 0.98 ferritin 2467
2004 Family JH.2 HFE2 (HJV) Testing hemojuvelin G320V Sat 0.26 ferritin 90 Undefined Sat 0.21 ferritin 26 21 19 Age 19 Sat 0.24 ferritin 30 Age 21 Sat 0.98 ferritin 2467 Age 19 Sat 1.00 ferritin 1403