Download

1 / 37
380 likes | 565 Views
Some survival basics. Developments from the Kaplan-Meier method October 29 2007. Kaplan-Meier Method. Nonparametric Estimation from Incomplete Observations E. L. Kaplan, Paul Meier Journal of the American Statistical Association , Vol. 53, No. 282 (Jun., 1958), pp. 457-481.

E N D
Some survival basics Developments from the Kaplan-Meier method October 29 2007
Kaplan-Meier Method • Nonparametric Estimation from Incomplete ObservationsE. L. Kaplan, Paul MeierJournal of the American Statistical Association, Vol. 53, No. 282 (Jun., 1958), pp. 457-481
Kaplan-Meier plot • Method estimates survival probabilities while accounting for withdrawals from the sample before the final outcome is observed • Graphical display to show the survival probabilities of ≥ 1 groups
Kaplan-Meier plot Example • After a heart attack, compare patient survival for those that underwent a procedure (Treatment group) vs. those who did not (No Treatment group) • The follow-up begins at the time of the heart attack but sometimes the procedure (Treatment) is not done immediately
Survival curves • Cox PH model with time-varying covariate to test but how to graphically display survival curves? • Some of the different approaches used: • Final covariate value • Reset start time • Extended Kaplan-Meier
* * Data example: Approach 1 Time
Approach 1: Final covariate value • Categorize patients by treatment completed by the end of follow-up • Some issues to consider: • Treatment bias patients not yet receiving the treatment are assigned to the treatment group • Survival bias survive long enough to receive treatment
* * Approach 1: Final covariate value Time
Data example: Approach 2 Time Where: = Time*0 for Treatment group
Approach 2: Reset start time • Include patients in the No Treatment group until they receive treatment • Censor them from No Treatment group • Add to Treatment group on day of treatment • The start time (t0) for No Treatment group is the beginning of follow-up. • The start time (t0 ) for Treatment group is date of treatment. • Underlying assumption: hazard rate in treatment group is constant over time
Approach 3: Extended Kaplan-Meier • Start patients in the no treatment group and switch the patient over after treatment • The start time (t0) is first day of follow-up for both groups. • No Treatment Group: • Include patients in the risk set until they receive Treatment • Censor patients at time of Treatment. • Treatment Group: • Add patients on the day they receive Treatment. • Patient at risk at time ti in Treatment group is Ni = Ni-1 – deaths – censored + new Treatment
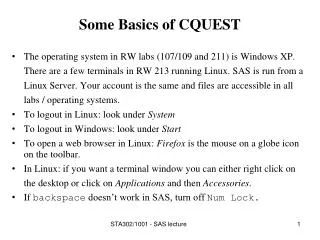
Comparison of approaches 1.00 0.95 Survival Probability 0.90 0.85 No Treatment (Approach 1 - Final covariate value) Treatment (Approach 1 - Final covariate value) No Treatment (Approach 2/3 - Reset start time/Extended KM) Treatment (Approach 2 - Reset start time) 0.80 Treatment (Approach 3 - Extended KM) 0 1 2 3 4 5 6 7 8 9 10 11 12 Time (months)
Approach 3: Extended KM • Advantage: • Consistency in Approach 3 and Cox proportional hazards model with time-varying covariate • Disadvantage: • Disadvantage of Approach 3: if too few patients with treatment at start of follow-up unstable estimate
Survival Tip #1: Proper Napping Position (from Worst Case Scenarios online http://www.worstcasescenarios.com/)
Survival Tip #2:How to Fend Off a Shark • Hit back. If a shark is coming toward you or attacks you, use anything you have in your possession—a camera, probe, harpoon gun, your fist—to hit the shark's eyes or gills, which are the areas most sensitive to pain. • Make quick, sharp, repeated jabs in these areas. (from Worst Case Scenarios online http://www.worstcasescenarios.com/)
Event (Competing Risk) Starting condition Event of Interest Example: Competing Risk
Introduction to Competing Risks • Interested in recurrence of an event in a time-to-event analysis • Prior to recurrence, death could occur Death is a competing risk to recurrence event • How to specify the outcome if recurrence is the event of interest? • Composite outcome - First event of either recurrence/death, censor on last follow-up • Censor on death and last follow-up
Assumptions for KM method • Survival probabilities are the same for patients entering into the study early or late • Actual event time is known • Patients who are censored have the same survival probabilities as those who continue to be followed
Non-Informative Censoring • The rate of event is similar for those who experience the event as those who did not due to censoring • What happens if there is informative censoring?
Example: Informative Censoring • Assume all event times are known for 10 patients • Patients either experience recurrence (event of interest) or death (competing risk) • No patients are lost to follow-up From: Grunkemeier G, Anderson R, et al. 1997. Time-related analysis of nonfatal heart valve complications: Cumulative incidence (Actual) versus Kaplan-Meier (Actuarial). Circulation. 96(9S):70II-74II.
Example: Informative Censoring D D R D R D R D R D D D D D D D R R R R R R R R D D D D D D 1.0 0.8 0.6 Freedom from Recurrence 0.4 0.2 0.0 0 2 4 6 8 10 Time
Note about informative censoring • Censored patients ‘withdrawn’ from risk set at time of censoring in KM method • However, censored patient is assumed to still have the same probability of experiencing the event of interest (non-informative censoring) • If patient is censored at time of death, KM estimation assumes this patient has the possibility of the recurrence
Competing Risks • When a patient can experience >1 type of event and the occurrence of one type of event modifies the probability of other types of events • Graphing based on using cumulative incidence function estimator
Example: Informative Censoring D D R D R D R D R D D D D D D D R R R R R R R R D D D D D D 1.0 0.8 0.6 Cumulative Incidence Function 0.4 0.2 0.0 0 2 4 6 8 10 Time
Cumulative incidence calculation in the presence of competing risks • Step 1: Calculate overall survival probability of being ‘event-free’, S(tj) • KM survival probabilities for assuming events include both event of interest as well as competing risk event(s)
Cumulative incidence calculation in the presence of competing risks • Step 2: Calculate cumulative probability of experiencing event of interest Step 2a: Calculate probability of failure for event of interest: h(tj)=1-(nj-dj)/nj=dj/nj where: nj=# patients at risk before time tj dj=# events of interest occurring at time tj
^ ^ ^ Σ F(t) = h(tj) * S(tj-1) all j, tj≤ t Cumulative incidence calculation in the presence of competing risks Step 2b: Calculate incidence of the event of interest: h(tj)*S(tj-1) • Cumulative incidence estimator at the end of the time,t = sum of the incidence in this interval and all previous intervals:
Cumulative incidence function approach to competing risks • The probability of any event happening can be partitioned into the probabilities for each type of event • For example, Frecurrence(t) + Fdeath(t) = 1- S(t) ^ ^ ^
^ ^ ^ F1(t) + F2(t) = 1-S(t) ^ F2(t) ^ F1(t) Cumulative Incidence Function Plot 0.25 Recurrence + Death Recurrence Death 0.20 0.15 Cumulative Incidence Function 0.10 0.05 0.00 0 100 200 300 Time (days)
Competing Risks • Graphical display • Comparing cumulative incidence functions for competing risk and event of interest • Comparing two or more groups for event of interest • Testing for differences • Tests to compare cumulative incidence between groups (similar to log-rank test) • Modeling to adjust for covariates (modification to Cox PH model)
Software • Cmprsk Package in R • Provides functions to plot, estimate, test, model • SAS Macro • Provides similar functions as in R • Downloadable from www.uhnresearch.ca/hypoxia/People_Pintilie.htm
References Survival curves with a time-dependent covariate • Simon R and Makuch RW. 1984. A non-parametric graphical representation of the relationship between survival and the occurrence of an event: application to responder versus non-responder bias. Statistics in Medicine. 3:35-44. • Feuer EJ, Hankey BF, et al. 1992. Graphical representation of survival curves associated with binary non-reversible time dependent covariate. Statistics in Medicine. 11:455-474. • Snapinn SM, Jiang Q, Iglewicz B. 2005. Illustrating the impact of a time-varying covariate with an extended Kaplan-Meier estimator. The American Statistician. 59(4):301-307. • Austin PC, Mamdani MM, et al. 2006. Quantifying the impact of survivor treatment bias in observational studies. Journal of Evaluation in Clinical Practice. 12(6):601-612. Competing risks • Pintilie, M. 2006. Competing Risks: A Practical Perspective. John Wiley & Sons Ltd. West Sussex, England. • Satagopan JM, Ben-Porat L et al. 2004. A note on competing risks in survival data analysis. British Journal of Cancer. 91:1229 -1235. • Grunkemeier G, Anderson R, et al. 1997. Time-related analysis of nonfatal heart valve complications: Cumulative incidence (Actual) versus Kaplan-Meier (Actuarial). Circulation. 96(9S):70II-74II. • Southern DA, Faris PD, et al. 2006. Kaplan-Meier methods yielding misleading results in competing risk scenarios. Journal of clinical epidemiology. 59:1110 -1114.