Download
1 / 149
1.59k likes | 2.03k Views
Radiation Hazards and Dosimetry. Dr. Craig Moore Medical Physicist & Radiation Protection Adviser Radiation Physics Service CHH Oncology. In the beginning.

E N D
Radiation Hazards and Dosimetry Dr. Craig Moore Medical Physicist & Radiation Protection Adviser Radiation Physics Service CHH Oncology
In the beginning ... • Wilhelm Roentgen discovered X-rays on 8th November 1895, and published his findings, "On A New Kind Of Rays" (Über eine neue Art von Strahlen), 50 days later on 28 December 1895 • Henri Becquerel discovered radioactivity on 26 February 1896 (“On the invisible rays emitted by phosphorescent bodies”. Comptes Rendus 122, 501–503, 1896)
First Human Radiograph • Frau Roentgen’s hand • Not medical - possibly to show off expensive gold ring??
First US medical radiograph • 3rd February 1896 by Edwin Frost an astronomer at Dartmouth College, New Hampshire. • A boy who had injured his wrist was seen by Dr. Gilman Duboi Frost, Edwin’s brother. • Edwin was asked to make the radiograph and produced the first image of a Colles fracture. (Remember, 3 months earlier no-one knew that X-rays even existed. Neither FDA nor NICE approval were required at the time.)
X-rays became all the rageAssumed to be no more harmful than light Dr Rome Wagner & glamorous assistant Unshielded Glass X-ray tube “Fluoroscope” - fluorescent screen inside black card
Early occupational exposures • Early X-ray tubes were gas filled and needed time to warm up after switching on • The X-ray pioneers took repeated X-rays of their own hands to see if the tube was ready for patients • X-ray tubes might be used like light bulbs to “illuminate” the room with X-rays
First Reports of Injury • (Nov 1985 Roentgen discovered X-rays) • March 1896 - The Lancet - L R L Bowen, in a talk to the London Camera Club, warned that x-rays might produce effects like sunburn • In April 1896 - BMJ - L G Stevens reported that people exposed to x-rays suffered sunburn and dermatitis
Early example In the summer of 1896 Herbert Hawks was demonstrating x-rays in Bloomingdale Brothers' Store in New York. Hawks, an assistant to Dr. Pupin at Columbia University, experienced radiation burns and received an unusual diagnosis “Mr. Hawks, during the afternoon and evening of each day for four days, was working around his apparatus for from 2-3 hours at a time. At the end of the four days, he was compelled to cease active work, owing to the physical effects of the x-rays upon his body. The first thing Mr. Hawks noticed was a drying of the skin, to which he paid no attention, but after a while it became so painful it was necessary to stop all operations. The hands began to swell and assumed the appearance of a very deep sunburn. At the end of two weeks the skin all came off the hands. The knuckles were especially affected, they being the sorest part of the hand. Among other effects were the following: the growth of the fingernails was stopped and the hair on the skin that was exposed to the rays all dropped out, especially on the face and sides of the head. The chest was also burned through the clothing, the burn resembling sunburn. Mr. Hawks' disabilities were such that he was compelled to suspend work for two weeks. He consulted physicians, who treated the case as one of parboiling.”
Association or Effect? • Hawks thought his injuries probably due to electrical effects, not X-rays • Others suggested that such effects came from • the electric sparks in the high-voltage generator, • from ultra-violet (uv) radiation, • from chemicals used in developing plates, • from ozone generation in the skin and • from faulty technique
Mounting evidence and early safety tip November 1896 Elihu Thomson purposely exposed the little finger of his left hand for half an hour close to an x-ray tube. Over a period of a week or two the finger became swollen, sensitive and painful. He was convinced that the effects were caused by the “chemical activity” of the rays and issued a caution. (One of his recommendations was “Do not expose more than one finger”)
Boston Medical & Surgical Journal, 1901 vol 144 page 173 - Rollins W. X-light kills. page 197 - Codman EA. No practical danger from the x-ray. Opinion was still divided William Rollins As early as 1902 Rollins wrote almost despairingly, that his warnings about the dangers involved in careless use of x-rays was not being heeded, either by industry or by his colleagues. By this time Rollins had proved that x-rays could kill experimental animals (inside a Faraday cage to prove it was not an electrical effect), could cause a pregnant guinea pig to abort, and that they could kill a foetus. He also stressed that "animals vary in susceptibility to the external action of X-light" and warned that these differences be considered when patients were treated by means of x-rays (Wikipedia)
First fatality from artificial radiation? Clarence Dally (glassblower & assistant to Thomas Edison, 1865–1904) By 1900, Clarence Dally was suffering radiation damage to his hands and face sufficient to require time off work. In 1902, one lesion on his left wrist was treated unsuccessfully with multiple skin grafts and eventually his left hand was amputated. An ulceration on his right hand necessitated the amputation of four fingers. These procedures failed to halt the progression of his carcinoma, and despite the amputation of his arms at the elbow and shoulder, he died from mediastinal cancer. Dally is thought to be the first American to die from the effects of experimentation with radiation. Following this, Thomas Edison abandoned his research on X-rays. In 1903, a shaken Edison said “Don't talk to me about X-rays, I am afraid of them.“ (Wikipedia) Glass X-ray tube in wooden box (to shield from high voltage electricity, not X-rays) “Fluoroscope” - fluorescent screen inside black card (The famous) Thomas Edison
So, were the X-ray Pioneers idiots? • We now know that a radiation dose of 4 Gray to the whole body will kill 50% of people within 30 days [ LD(50/30) = 4 Gy ], but • 4 Gray of energy is 4 Joules per kg • 4 Gy to whole body is enough to raise body temperature by only around 0.001oC • i.e. less heating effect than a sip from a cup of hot tea • 19th century scientists knew how much electrical energy they were using to make X-rays, so knew amount of energy was trivial • Cancer risk difficult to determine when “natural” incidence of cancer so high • Also, no knowledge of DNA and effect of ionisation on cell.
First Radiotherapy TreatmentEmil Herman Grubbé • Not all bad news! • 29th January 1896 • Woman (50) with breast cancer • 18 daily 1-hour irradiation • Condition was relieved, although died shortly afterwards from metastases.
Aside First Cardiac Catheterisation • 1929 Werner Forßman - • inserting cannula in vein in own arm, through which he passed a catheter for 65 cm • then walked to the X-ray department, where a photograph was taken of the catheter lying in his right auricle. • From Wikipedia - In 1929, while working in Eberswalde, he performed the first human cardiac catheterisation. He ignored his department chief and persuaded the OR nurse in charge of the sterile supplies, Gerda Ditzen, to assist him. She agreed, but only on the promise that he would do it on her rather than on himself. However Forssmann tricked her by restraining her to the operating table and pretending to locally anaesthetise and cut her arm whilst actually doing it on himself. He anesthetized his own lower arm in the cubical region and inserted a uretic catheter into his antecubital vein, threading it partly along before releasing Ditzen (who at this point realised the catheter was not in her arm) and telling her to call the X-Ray department. They walked some distance to the X-ray department on the floor below where under the guidance of a fluoroscope he advanced the catheter the full 60 cm into his right ventricular cavity. This was then recorded on X-Ray film showing the catheter laying in his right atrium. • The head clinician at Eberswalde, although initially very annoyed, recognized Werner's discovery when shown the X-rays; he allowed Forssmann to carry out another catheterisation on a terminally ill woman whose condition improved after being given drugs in this way
Radiation Injury Recognised • By 1910 most workers using X-rays and radioactive substances were taking some precautions such as • shielding the tube to produce a collimated beam • lead-rubber protective wear for operators • using a phantom hand to check tube rather than operator’s hand • filtering the beam to remove soft X-rays • Sadly too late for some. In 1936 a memorial stone was unveiled in Hamburg to 160 medical men, physicists, chemists, laboratory workers and nurses from 15 nations whose deaths were due to working with X-rays with the citation, “They were heroic pioneers for a safe and successful application of x-rays to medicine. The fame of their deeds is immortal.”
Protection Progress • 1898 Roentgen Society Committee of Inquiry • 1915 Roentgen Society publishes recommendations • 1921 British X-Ray and Radiation Protection Committee established and reported • 1928 2nd International Congress of Radiology adopts British recommendations + the Roentgen • 1931 USACXRP publishes first recommendations (0.2 Roentgens per day) • 1934 4th ICR adopts 0.2 Roentgens per day limit • Note, • 0.2 Roentgens per day 500 millisieverts per year, which is the current legal skin dose limit. • Risk of skin burns was well understood in early 20th century • Whether radiation induced cancer was still a matter of debate
Atomic Bombs • Two A-bombs detonated above Hiroshima and Nagasaki, Japan in August 1945 • Within the first 4 months, the acute effects killed 90,000–166,000 people in Hiroshima and 60,000–80,000 in Nagasaki, with roughly half of the deaths in each city occurring on the first day • Estimate of the total immediate and short term cause of death
Radiation Effects • Acute radiation syndrome • Including vomiting, diarrhea, reduction in the number of blood cells, bleeding, epilation (hair loss), temporary sterility in males, and lens opacity (clouding ) • Late 1940’s Dr Takuso Yamawaki noted an increase in leukaemia • 20% of radiation cancers were leukaemia (normal incidence 4%) • Incidence peaked at 6-8 years • Solid cancers – excess seen from 10 years onwards.
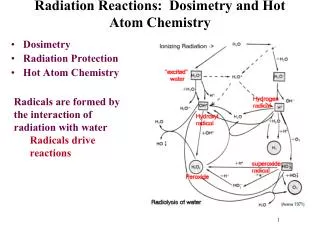
Ionising Radiation - + Ionising radiations – have the ability to separate electrons from atoms to produce “ions”
Radiation Hazards Why is it dangerous?
Damage depends on a number of factors: • The type and number of nucleic acid bonds that are broken • The intensity and type of radiation • The time between exposures • The ability of the cell to repair the damage • The stage of the cell’s reproductive cycle when irradiated
Aside: Quantifying Radiation, to quantifying the risk
Absorbed Dose (D) • Amount of energy absorbed per unit mass [D=d/dm] • 1 Gray (Gy) = 1 J/kg • Specific to the material, e.g. • absorbed dose to water • absorbed dose to air • absorbed dose to bone • Can be relatively easily measured with a “dose meter”
Typical Values of D • Radiotherapy dose = 40 Gy to tumour (over several weeks) • LD(50/30) = 4 Gy to whole body (single dose) • Typical 1 minute screening = 20 mGy skin dose • Chest PA = 160 mGy entrance surface dose .
Different radiations, different risk • 1 Gy of alpha particle radiation produced more tissue damage than • 1 Gy of neutron radiation, which produces more tissue damage than • 1 Gy of X-rays • Multiplying ABSORBED DOSE in Gy by a weighting factor (wR) for the relative damage cause by different radiations gives us EQUIVALENT DOSE
Equivalent Dose (HT,R) • Absorbed dose to tissue x radiation weighting factor • In mathematical notation • HT,R = wR.DT,R • or if exposed a mix of radiations HT = R wR.DT,R • (T = which tissue or organ you are considering; R = which type pf radiation) • Units are Sieverts (Sv) Professor Rolf Sievert (1896 – 1966) was a medical physicist whose major contribution was in the study of the biological effects of radiation.
Equivalent Dose (HT,R)weighting factors, wR • HT,R = wR.DT,R • wR = 1 for • all photons (e.g. X-rays and gamma rays used in nuclear medicine), • electrons (e.g. beta particles used for nuclear medicine therapy and electron beams used in radiotherapy) and • muons (not used in medicine), • wR = 5-20 for neutrons, (depending on energy) • wR = 5 for protons (beginning to be used in radiotherapy), • wR = 20 for alpha () particles (recently used for palliative nuclear medicine therapy), • e.g. for X-rays 1 Gy = 1 Sv, but for alpha particles 1 Gy = 20 Sv.
Equivalent Doseexample of use • Legal dose limits for skin or lens of eye exposure are expressed as EQUIVALENT DOSE • lens of eye limit for radiation workers = 150 mSv equivalent dose per calendar year • Limit for any 1 cm2 of skin of radiation workers = 500 mSv equivalent dose per calendar year
Different organs or tissues, different risk • Also, 1 Sv to whole body is more likely to induce cancer than 1 Sv just to the head, etc. • We need a quantity which is proportional to the overall risk of inducing cancer - EFFECTIVE DOSE • 1 Sv equivalent dose to the lung is more likely to induce cancer than • 1 Sv equivalent dose to the thyroid, which is more likely to induce cancer than • 1 Sv equivalent dose to the brain
Effective Dose (E) • Sum of equivalent doses to each tissue/organ x organ weighting factors wT • E = TwT.HT • Units are Sieverts (Sv) • You need to know the dose to each organ/tissue of interest.
wT = 12% for red bone marrow, breast, colon, lung, stomach, wT = 8% for gonads wT = 4% for liver, oesophagus, thyroid, bladder wT = 1% for skin, bone surfaces, brain, salivary glands wT = 12% for average dose to remainder tissues - adrenals, extrathoracic region, gall bladder, heart, kidneys, lymphatic nodes, muscle, oral mucosa, pancrease, prostate, small intestine, spleen, thymus, uterus/cervix ICRP Publication 103 (2007)tissue weighting factors
Example of effective dose • Abdomen PA radiograph • 80 kVp • 2.5 mm Al filtration • 75 cm FSD • 35 x 43 cm film • 5.4 mGy entrance skin dose • From this data computational models can be used to calculate the organ doses for an average man/woman • Weighting factors can be applied • The results added together give us EFFECTIVE DOSE
What’s effective dose for? • Organ doses ranged • from 0.00 mSv (brain, thyroid) • to 2.97 mSv (kidneys) • Effective dose was 0.36 mSv • Risk of inducing cancer risk of 0.36 mSv to all organs/tissues.
Effective dose example • Effective dose calculated for abdomen PA radiograph = 0.36 mSv • Therefore, risk of cancer from abdomen PA is the same as an equivalent dose of 0.36 mSv to the whole body
Typical Values of E (X-ray examinations) • Barium enema = 7 mSv • CT abdomen = 10 mSv • Conventional abdomen = 1.0 mSv • Chest PA = 20 mSv • Pulmonary angiography = 5.4 mSv • Annual effective dose limit for radiation workers = 20 mSv • Annual background dose = 2.5 mSv.
Concept of Absorbed Dose in Nuclear Medicine The calculation of the absorbed dose - a tricky problem,because of several factors: • 1. the distribution of the radionuclide within the body and its uptake in certain critical organs • 2. inhomogeneous distribution of the nuclide even within the critical organ • 3. the biological half-life of the nuclide, which may vary with patients' ages and may be modified by disease or pathological conditions.
Absorbed dose to an organ is determined by: • Radionuclide • Activity administered • Activity in the organ • Size and shape of the organ • Activity in other organs • Kinetics of radiopharmaceutical • Quality of radiopharmaceutical
The MIRD System of Internal Absorbed Dose Calculation • MIRD- Medical Internal Radiation Dosimetry developed by the Society of Nuclear Medicine • The organ containing the radionuclide is called the source organ – this accumulates the activity • We wish to calculate the absorbed dose to the targetorgan – this is irradiated by activity in the source organ • The source and target organs may be the same • The amount of radiation from the source reaching the target must be known
Derivation of the General MIRD Equation • Let E be the mean energy per particle (photon or electron) • If n is the number of particles emitted per disintegration • then nE is the mean energy emitted per disintegration
Absorbed Dose • Energy absorbed in a material per unit mass • Has unit of the gray (1 Gy = 1 J/kg)