Download
1 / 47
470 likes | 602 Views
Acute Musculotendinous Injuries of the Shoulder. April 7, 2008 Taylor Brown, M.D. Basic Themes. Restore normal anatomy if the patient is an acceptable risk for surgery. Basic Themes. Repair is most easily completed within the first weeks after injury. Basic Themes.

E N D
Acute Musculotendinous Injuries of the Shoulder April 7, 2008 Taylor Brown, M.D.
Basic Themes • Restore normal anatomy if the patient is an acceptable risk for surgery
Basic Themes • Repair is most easily completed within the first weeks after injury
Basic Themes • Injury occurs with sudden forceful overload of a maximally contracted muscle
Basic Themes • Associated with steroid use • Associated with weightlifters and bodybuilders • Associated with weightlifters and bodybuilders who use steroids
Common Injuries • Rotator Cuff • Biceps Brachii Long Head
Less Common Injuries • Pectoralis Major
Reportable Injuries • Deltoid • Latisimus Dorsi • Coracobrachialis • Biceps Brachii Short Head • Pectoralis minor
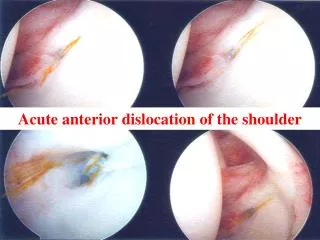
Acute Rotator Cuff Tears • Associated with a distinct trauma • Fall or Near Fall • Lifting or Catching a heavy or falling object • Subluxation or dislocation
Acute Rotator Cuff Tears • Suspect with any persistent loss of abduction or forward elevation 2 weeks after a seemingly benign trauma • Diagnose with early MRI
Acute Rotator Cuff Tears • Usually a large tear of supraspinatus and infraspinatus
Acute Rotator Cuff Tears • Carefully evaluate subscapularis with belly press or bear hug • lift off test usually impossible
Acute Rotator Cuff Tears • Repair acutely within first several months to obtain the best outcome • fatty degeneration • Tissue contracture
Acute Rotator Cuff Tears • Fatty degeneration present within first 4 months after an acute tear
Acute Rotator Cuff Tears • Fatty degeneration does not reverse, even with a successful repair • Fatty degeneration, however, does not preclude a successful outcome
Acute Rotator Cuff Tears • Tissue contracture, if present, requires specific soft tissue releases • Coracohumeral ligament • Capsule between cuff and glenoid neck • You can bill an appropriate code for soft tissue releases associated with large, retracted cuff tears • Lysis of adhesions 29825 Bert and Beach
Acute Rotator Cuff Tears • Carefuly evaluate tear pattern • “L” shaped tear crescent
Acute Rotator Cuff Tears • Go forward with your standard arthroscopic rotator cuff repair Single row Dual row Convergence
Acute Rotator Cuff Tears • Postoperative protocol • Use your usual protocol for a large tear • Pillow sling 6 to 8 weeks • Avoid strengthening for at least 3 months
Acute Rotator Cuff Tears • Nonoperative care of large tears • Counsel patient regarding expectations • Persistent loss of function • Possible pseudoparalytic shoulder • Possible rotator cuff arthropathy
Biceps Long Head Rupture • Popeye deformity • Bimodal distribution • 40 year old heavy laboring or active man • 70 year old former or persistent laboring man
Biceps Long Head Rupture • Diagnose with • History of painful pop • Deformity and ecchymosis on exam • MRI to confirm diagnosis and evaluate rotator cuff
Biceps Long Head Rupture • Nonoperative treatment • Persistent deformity • Persistent loss of supination strength (10-20%) • Most appropriate for older age group • Chronic spasm or ache (s. snyder)
Biceps Long Head Rupture • Subpectoral Tenodesis • Accurate restoration of length • Cosmetically appealing • Removes diseased portion of tendon • easy
Biceps Long Head Rupture • Subpectoral Tenodesis • Accurate restoration of length • Proximal musculotendinous junction placed at inferior border of pectoralis major tendon
Biceps Long Head Rupture • Subpectoral Tenodesis • Cosmetically appealing • Axillary fold incision and scar • Restoration of biceps contour
Biceps Long Head Rupture • Subpectoral Tenodesis • 3 cm axillary fold incision • Blunt dissection directly toward humerus • Palpate inferior border of pectoralis tendon • Blunt hohman retractor laterally elevates pectoralis tendon • Chandler medially to protect neurovascular structures
Biceps Long Head Rupture • Subpectoral Tenodesis • Withdraw biceps tendon from groove or anterior arm • Remove all of diseased tendon except 15mm just proximal to musculotendinous junction • Weave permanent stitch through tendon • ACL guidewire into groove 5mm above inferior border of pec tendon
Biceps Long Head Rupture • Subpectoral Tenodesis • Acorn reamer over guidewire through one cortex only • Usually 6.5mm wide socket • Seat tendon within socket and drive 6.25 x 15mm screw down over biotenodesis driver
Biceps Long Head Rupture • Subpectoral Tenodesis • Suture anchors have been used as well • Mitek G2 or G4
Biceps Long Head Rupture • Subpectoral Tenodesis • Keyhole technique
Biceps Long Head Rupture • Subpectoral Tenodesis • Complications • Loss of tendon fixation • Fracture at screw site • Persistent defect at PLLA screw site
Biceps Long Head Rupture • Humeral Head Fixation • Requires open approach to identify biceps tendon distally in arm • Suture passer is fed through bicipital groove to retrieve tendon • Fixed at humeral head with Biotenodesis screw or suture anchors
Biceps Long Head Rupture • Humeral Head Fixation • Hard to do • May end up maintaining diseased tendon
Biceps Long Head Rupture • associated partial or full thickness rotator cuff tears which may have caused prodromal symptoms • Fix it at the same setting
Biceps Long Head Rupture • Postoperative protocol • Sling for 2 to 4 weeks • Begin passive and active assist motion immediately • Avoid heavy lifting for 6 weeks • More commonly limited by associated rotator cuff repair
Pectoralis Major Tear • Cosmetic and Functional Deformity • Young to Middle age male weightlifters
Pectoralis Major Tear • Diagnose with • History of painful pop • Thin anterior axillary fold on exam • Visual deformity • MRI to confirm exact location of injury (tendon versus muscle belly)
Pectoralis Major Tear • Nonoperative care for • Partial tears • Muscle belly ruptures
Pectoralis Major Tear • Operative Repair • tendon avulsions from bone • most easily achieved in first weeks following injury • Open anterior axillary fold incision
Pectoralis Major Tear • Weave permanent stitches through tendon • Anchor to lateral ridge of bicipital groove with bone tunnels or suture anchors
Deltoid Rupture • Acute traumatic rupture • Reportable • No published treatment regimen
Deltoid Rupture • More commonly, a postoperative complication from open shoulder surgery • Reportedly very difficult to obtain a solid repair with permanent sutures woven through muscle and acromial bone tunnels • May benefit from patch augmentation
Latissimus Dorsi Tear • 4 tears reported in the literature • Combined anterior and posterior approaches • Repair with suture anchors to medial ridge of bicipital groove • Beware of axillary neurovascular bundle
Coracobrachialis Tear • Have not seen it • 2 cases reported
Pectoralis Minor Tear • Have not seen it • 1 case report
Questions? St. Luke’s Orthopedic Symposium “Sports Medicine and the Team Physician” The Houstonian April 11-12, 2008 www.sleh.com/orthosymposium