Download
1 / 13
130 likes | 804 Views
The Difficult and Failed Airway. Principles of Rapid Sequence Intubation Jason Carter, B.S., L.P. I. The Difficult Airway. Defined Difficult to oxygenate and ventilate Difficult to intubate Difficult to perform a cricothyroidotomy. B. Predicting the Difficult Airway. LEMON law

E N D
The Difficult and Failed Airway Principles of Rapid Sequence Intubation Jason Carter, B.S., L.P.
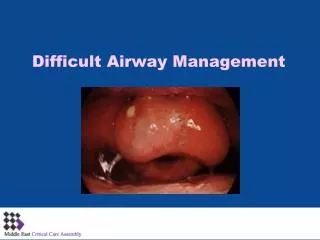
I. The Difficult Airway • Defined • Difficult to oxygenate and ventilate • Difficult to intubate • Difficult to perform a cricothyroidotomy
B. Predicting the Difficult Airway LEMON law • Look externally • Evaluate the 3-3-2 rule • Mallampati classification • Obstruction ? • Neck Mobility
Beard or Moustache that hinders seal of BVM Abnormal Facial Shape Extreme cachexia Endentulous mouth with sunken cheeks Disruption of the lower face due to trauma. Large central incisors High-arching palate Receding mandible Short bull neck Morbid obesity 1. Look externally
2. Evaluate the 3-3-2 Rule • Three finger mouth opening • Three finger mentum-to-hyoid • Two finger floor-of-mouth-to-thyroid cartilage
3. Mallampati classification • Spaciousness of mouth • Done sitting with head in sniffing position, mouth wide open and tongue sticking out
4. Obstruction • Foreign object – Magill forceps • Laryngeal tumor • Known or suspected epiglottitis • Known or suspected peritonsillar abscess • Direct airway trauma • Extrinsic airway hematoma with compression
5. Neck mobility • Spinal motion restriction automatically makes the RSI difficult • Non-trauma patients should be able to bring their head into the sniffing position
II. Clinical Approach to the Difficult Airway • First complication is mechanics • Worst is esophageal intubation • Factors in failure vs. success
A. Clinical Techniques • Re-position the head – non-traumatic • Jaw Lift in trauma patients • Miller blade for epiglottis • BURP technique • Leave inadvertent esophageal tube in place • 1 – 1.5 size smaller ETT
III. The Failed Airway • Failed airway defined • failure of single attempt at oral intubation followed by inability to maintain SpO2 90% with BVM • Three failed attempts made by an experienced airway manager
B. Management of the Failed Airway • “Can’t intubate, can oxygenate” has time • CombiTube Placement • Digital Intubation • Smaller tube • BURP • “Can’t intubate, cannot oxygenate” immediate response • Needle or Surgical Cricothyroidotomy
Conclusion • General Rule—prepare for the worst and hope for the best • Before RSI, determine difficulty of intubation using LEMON law • All Spinal Motion Restriction patients are automatically difficult • Keep up intubation skills