Download
1 / 24
870 likes | 3.42k Views
Hysteroscopy. Dr Nasira Sabiha Dawood. Endoscopy : Types. Laparoscopy Colposcopy Hysteroscopy Falloscopy Amnioscopy Fetoscopy. Hysteroscopy. Viewing and operating in the endometrial cavity through transcervical approach by instrument called hysteroscope. History.

E N D
Hysteroscopy Dr Nasira Sabiha Dawood
Endoscopy : Types Laparoscopy Colposcopy Hysteroscopy Falloscopy Amnioscopy Fetoscopy
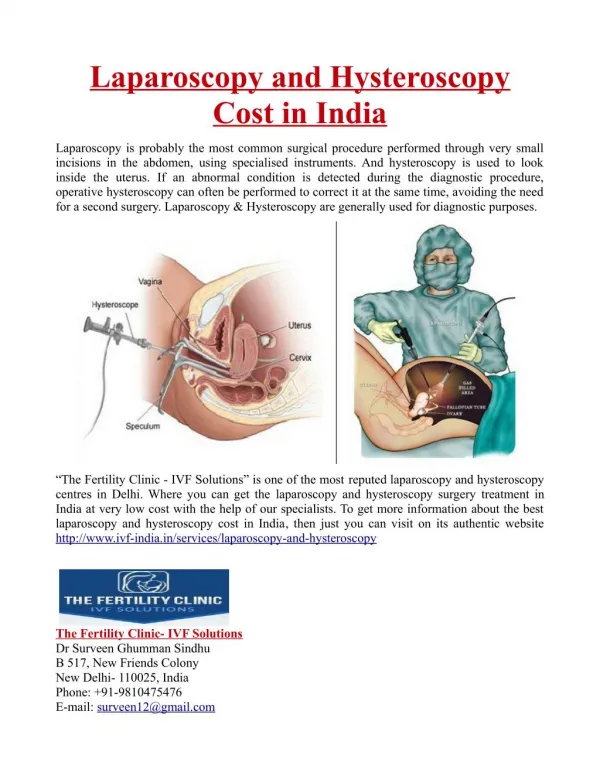
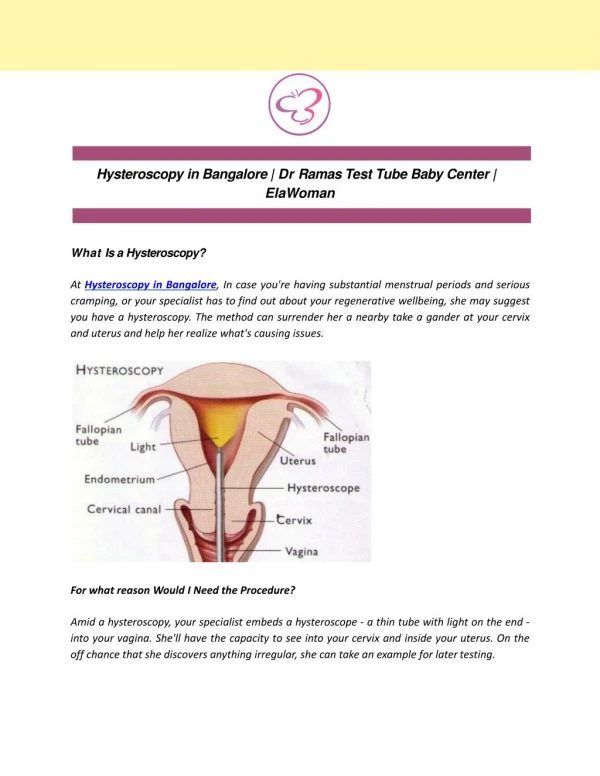
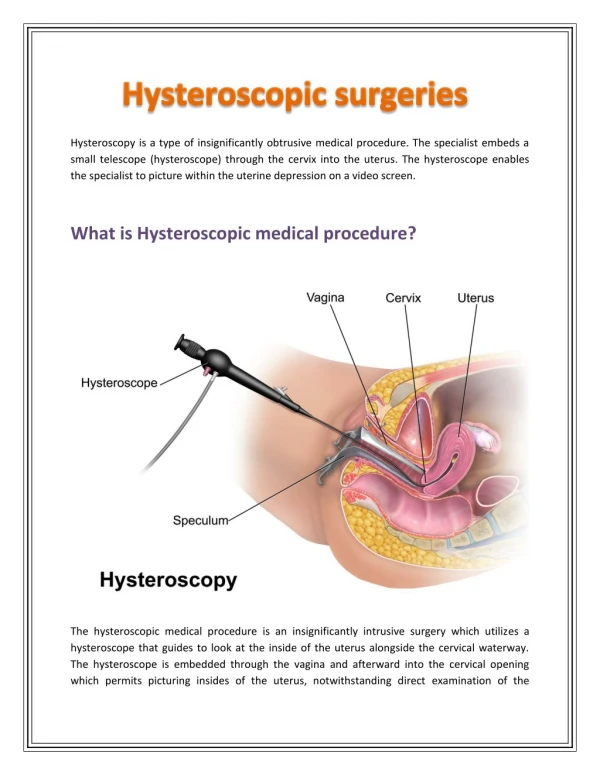
Hysteroscopy Viewing and operating in the endometrial cavity through transcervical approach by instrument called hysteroscope
History 1805 Bozzini used candle light for illumination 1869 Pantaleoni, first described the procedure
Hysteroscopy Hysteroscopy as described by S.Duplay and S.Clado, 1898
History 1925 Rubin first used CO2 to distend the uterus 1938 Gauss used fluids to achieve uterine expansion 1970s More practical and usable instruments 1980s Liquid distention media became routine mid-1980s Hysteroscopic procedures nearly replaced D&C Past decades, refinements in the areas of Optics Fiberoptic technology Surgical accessories Visual resolution and surgical techniques Novel instruments and techniques continue to emerge
Hysteroscopy Minimally invasive intervention Diagnosis instant Treatment Out patient procedure Part of CPSP/RCOG core training Diagnostic and operative hysteroscopy a standard procedure in gynaecologic practice due to its safety and efficacy
Components A rigid or flexible tube A light delivery system Light source outside the body Optical fiber system A lens system transmitting the image Viewer Additional channel for Medical instruments Manipulators
Rigid hysteroscope Most common Wide range of diameters narrow (3-5 mm), sharpest and clearest view, minimal cervical dilation, well tolerated, paracervical block larger (8-10 mm), increased cervical dilation, in operating room, intravenous (IV) sedation or general anaesthesia Large, outer sheath for media and surgical instruments
Flexible hysteroscope Office hysteroscopy Flexibility Range 120-160° Irregularly shaped uterus Navigate around intrauterine lesions More easy insertion Flexible contour accommodates to cervix
Light source Internal or external light source Illumination at distal tip Energy sources Tungsten Metal halide Xenon (superior option)
Gases Carbon dioxide (CO2) Hysteroscopic insufflator required regulate flow limit maximal intrauterine pressure
Fluids Symmetric distention Flush blood, mucus, bubbles, and tissue fragments Closed systems actively return fluid to a pump and reservoir Open systems allow free flow of medium out into a collection bag for volume monitoring 0.9% sodium chloride and lactated Ringer solution 5% Mannitol 3% sorbitol 1.5% glycine Dextran 70
Energy sources Monopolar cautery Resectoscope Monopolar, double-armed electrode and a trigger device cuts and coagulates Depth of thermal damage based on Endometrial thickness Speed, pressure, and duration of contact Power setting Bipolar cautery Laser techniques Fiberoptic lasers Potassium-titanyl-phosphate (KTP) Argon Nd:YAG lasers
Surgical instruments Scissors Biopsy forceps Grasping instruments Roller ball Loop electrode Scalpel Resectoscope with suction channel and pump Hysteroscopic morcellator
Indications Abnormal uterine bleeding Infertility Recurrent miscarriages Intrauterine adhesions Müllerian anomalies approx 1-2% of all women, 4% of infertile women, and 10-15% with recurrent miscarriage Polyps and fibroids Proximal tubal obstruction Intrauterine devices
Contraindications Cervical or uterine infection Uterine cavity >10 cm Severe medical conditions Pregnancy Cervical cancer
Preoperative preparation Laboratory Investigations CBC/ Blood typing Viral screening Electrolytes HVS/Cervical cultures Pap smear Imaging Studies Hysterosalpingogram or sonohysterogram CT scanning or MRI are not usually needed
Procedure Anaesthesia Positioning Bladder catheterization Pelvic examination under anaesthesia Cervical dilatation Placing the Hysteroscope Visualization of the uterine cavity
Complications Few, Minor, Rare Infection Uterine/cervical trauma/perforation endoscope biopsy instrument Bleeding Media-related complications Gas embolism Fluid overload Electrolyte imbalance
Follow-up Follow-up in 2-4 weeks
Progress at FFH No obstetric unit in FFH before Aug 2000 Nov 2000 Plan finalised for obstetric Unit Feb 2001 Founder Principal FUMC - Vision 2010 Jan 2002 Obstetric Unit established in FFH First obstetric case (SVD) Sep 2006 Hysteroscope received Jan 2009 Hysteroscope in regular use