Download
1 / 46
500 likes | 942 Views
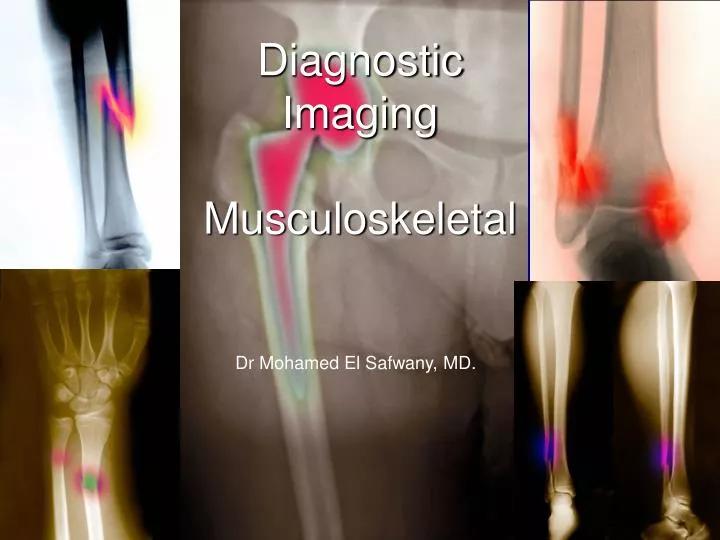
Diagnostic Imaging Musculoskeletal. Dr Mohamed El Safwany, MD. Intended learning Outcomes. The student at the end of this lecture should be able to recognize : Sprains (ligamentous injuries), Strains ( musculotendinous injuries), Meniscal injuries, Fractures , and Dislocations .

E N D
Diagnostic ImagingMusculoskeletal Dr Mohamed El Safwany, MD.
Intended learning Outcomes The student at the end of this lecture should be able to recognize : • Sprains (ligamentous injuries), • Strains (musculotendinous injuries), • Meniscal injuries, • Fractures, and • Dislocations.
Musculoskeletal Injuries • Musculoskeletetal problems commonly occur as a result of both serious athletic pursuits and activities of daily living. • Most sports injuries are the results of: • contusions, • sprains (ligamentous injuries), • strains (musculotendinous injuries), • meniscal injuries, • bursitis, • fractures, and • dislocations. • Physical therapy is an important adjunct to the management of these disorders
Skeletal Imaging • Majority are diagnosed by plain radiograph • AP and Lateral projections • Oblique views for trauma involving joints, hands and feet • CT - fine bone structure ( skull,spine and pelvis) • MRI - evaluation of soft tissue • Nuclear medicine - bone metastases, osteomyelitis and occult trauma (stress fractures)
Skeletal Imaging • Most bone lesions are obvious on clinical history • >95 % bone films are obtained for: • Evaluation of trauma • Eval. Arthritis • Eval. Degenerative conditions • Metastases
Sprains • Sprains are ligament injuries. • Ligaments attach bone to bone • Ligaments are like strong cords, tough and elastic, and provide stability and strengthbetween joints, but when pulled or stretched to their limit they can tear or rupture. • Depending on the amount of ligament tearing, a sprain can be mild, moderate, or severe. • An alternate classification is; a first-degree, second-degree or third-degree sprain.
Sprains 1rst degree - joint pain / tenderness - no laxity 2nd degree - joint laxity present - pain and tenderness 3rd degree - ligament broken - unstable joint
Sprains • Most sprains are associated with varying degrees of pain, swelling and impairment of range-of-motion or weight bearing. • The most commonly involved areas are the shoulder, the elbow, the knee and the ankle. • Knee and ankle sprains are among the most common of all sports injuries. • If the physical exam is difficult to perform or damage to other intra-articular structures is suspected, Ultrasound and MRI can help determine the full extent of injury.
Strains • A strain is the tearing of a muscle-tendon unit. • termed tendonitis • acute or chronic • caused by overuse or a single episode of overactivity • pain results from minor tears in the tendons, from accumulated injuries (repetitive micro-trauma) that outpace the body’s ability to repair itself.
Strains • May result in pathologic changes of the soft-tissue and bones: • tendon degeneration, osteophytes, stress fractures, or nerve entrapment. • also graded as mild, moderate or severe. • Severe strains are characterized by rupture of any part of the tendon complex e.g biceps, patella or Achilles. • Diagnosed by Ultrasound and MRI.
Terminology • Fractureis a break or loss of structural continuity in a bone. • it is important that fractures be described in a precise and detailed manner. • Dislocation and Subluxation alters the normal relationship between joint surfaces. • Dislocation :the normally apposing joint surfaces completelyloose contact • Subluxation :those surfaces are only partially separated.
Fractures are described • Description
Fracture • displacement
Fracture • Angulation dorsal volar
Fracture • Rotation
Fracture • Bayoneting
Fracture • Distraction
Fracture • Oblique
Fracture • Greenstick
Fracture • Transverse
Fracture • Comminuted
Fracture • Spiral
Fracture • Dislocation
Fracture • Nonunion Malunion
Fracture • Avulsion
Fractures • Fractures are open or closed. • Open: break in the surrounding skin or mucosa that allows the fracture to communicate with the external environment. • Open fractures are graded 1-3, with 3 being the most severe, and having the highest incidence of complications (e.g. osteomyelitis and nonunion).
Open fractures • Grade 1: wounds < 1cm in length • Grade 2: wounds > 1cm in length but clean w/o devitalization of tissue • Grade 3: wounds > 1 cm in length, grossly contaminated, associated with comminuted fractures and vascular injury.
Fracture Description • Fractures are further described based on: • Location • Pattern • Displacement • When describing location, • the bone affected is identified • as well as the specific part of the bone involved (proximal or distal epiphysis,etc.)
Fracture Pattern • The fracture pattern relates to fracture geometry, which suggests the type and amount of kinetic energy the bone has been subjected too. • A transverse fracture is a low-energy injury, usually the result of either a direct blow to a long bone or a ligament avulsion. • An example is a “night stick” fracture, which involves the ulna and occurs when the forearm is used to defend against an assault. • Stress and pathologic fractures usually have a transverse pattern.
Fracture Pattern • Spiral or obliquefractures result from a rotatory or twisting injury. • These fractures have a tendency to displace after reduction and immobilization. • Spiral or oblique fractures typically require ORIF. • A fracture with two or more fragments is termed comminuted.
Fracture Pattern • An impacted fracture is commonly seen in metaphyseal bone, such as the femoral neck, the distal radius or tibial plateau fractures. • These (impacted) are low-energy injuries in which two bone fragments are jammed together. • Fractured bone fragments can be displaced due to the force of the injury, gravity, or muscle pull. • Displacement is described in terms of angulation, rotation and length.
Salter-Harris (Growth Plate) Fractures • Growth plate fractures in children are based on the Salter-Harris classification of injuries. • Growth plate injuries, no matter how trivial, have the potential to cause growth disturbance of the involved bone. • These fractures are classified as type I-V.
Salter-Harris Classification Type I- through the physis. Type II- through the physis and metaphysis. Type III- through the physis and epiphysis. Type IV- through the physis, metaphysis and epiphysis. Type V- crush injury to the physis.
Principles of fracture management: • Patients with fractures should be managed as trauma patients. • always check for associated injuries. • Next, assess the neuro-vascular status. • Remember to check : • distal pulses and capillary refill. • sensory and motor function (distal to the fracture )
Fracture management • The three principles of fracture care involve: 1) Reduction of deformity 2) Maintenance of reduction 3) Rehabilitation of function
Closed reduction • Reduction • Closed • Open • Closed reduction: involves the manual manipulation of the fracture into a functional position. • traction is applied • deforming forces are reversed • realign the bone fragments.
Open reduction • open reduction • fracture is surgically exposed • bone fragments are manipulated directly (ORIF=open reduction and internal fixation). • Open reduction indicated when: • closed reduction methods fail • with intra/articular fractures (joint surface must be aligned anatomically to prevent the development of posttraumatic arthritis.
Maintaining alignment • Maintaining alignment requires • Immobilization: • include casting, splinting, traction, functional bracing, and internal or external fixation. • The type of immobilization depends upon fracture stability. • Splints and casts immobilize and support the injured extremity and thereby reduce pain • Splinting and casting are also used postoperatively to provide additional stabilization.
Splinting and casting • Splinting and casting accomplished with plaster or synthetic materials such as fiberglass. • Splints differ from casts in that splints are not circumferential and thus allow swelling of the extremity without a significant increase in pressure within the splint. • Swelling within the cast increases pressure, potentially resulting in a compartment syndrome or pressure sores.
Splinting and casting • Many of the fundamental rules of splinting and casting are identical. • Ideally, at least one joint proximal and one joint distal to the injury are immobilized. • Prior to immobilization, fractures are reduced, and, as much as possible are placed in a position of function. • The extremity and bony prominences are padded to prevent pressure sores and neurovascular compression.
Complications • Common complications of musculoskeletal injuries: • ARDS (fat embolism) • DVT • Atelectasis • Nerve compression • Osteomyelitis
Assignment • 5 students will be selected for assignments.
Suggested Readings • David Sutton’s Radiology
Questions State Salter Harris fracture Classification of children.