Download
1 / 34
350 likes | 776 Views
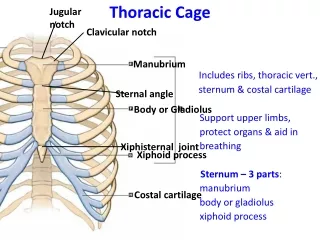
PLIF with cage alone. 최우진 , 안형준 , 전기현 , 김현성 , 김관태 Department of neurosurgery, Hurisarang Spine Hospital Daejeon , Korea. Lumbar Interbody fusion. Cloward introduced PLIF in 1953 Transforaminal LIF ( TLIF ) Anterior LIF ( ALIF ) Microendoscopic LIF Percutaneous endoscopic LIF

E N D
PLIF with cage alone 최우진,안형준,전기현,김현성,김관태 Department of neurosurgery, Hurisarang Spine Hospital Daejeon, Korea
Lumbar Interbody fusion • Cloward introduced PLIF in 1953 • Transforaminal LIF ( TLIF ) • Anterior LIF ( ALIF ) • Microendoscopic LIF • Percutaneous endoscopic LIF Usually combined with pedicle screw
PLIF with cage alone • From 1998 to 2008 1092 PLIF patients with only a cage During the period, we had performed almost lumbar fusion surgeries with only a cage without pedicle screw fixation.
Introduction • Postero-lateral region of the endplate provides the greatest resistance to subsidence while the central region provides the least resistance. (Spine 2004, Lowe thomas G. MD) • Proper preparation of the endplate prevents subsidence and increases fusion rate ( complete removal of cartilaginous endplate, complete preservation of bony cortex. ) ( spine 2003, Oxland TR)
Large Cage • Interbody fusion cages with larger area of contact between cage and vertebral endplate produces a lower stress distribution pattern. ( Spine 2005 Kumar, Naresh MS ) • A larger diameter solid support has the greater maximun load of failure and the lower the risk of subsidence. (Spine 2004, Lowe thomas G. MD) • The load-bearing capabilities of the open box cage are superior to those of the fenestrated tube cage (Spine 2006 Matsumura, Akira MD)
local bone chipVs Allo-bone, iliac bone , hydroxyapatate block, BMP • PLIF using cages impacted with laminar bone chips is a useful method when considering the time required for surgery and the morbidity of the autograft donner sites. (Spine 2005 Kim, K S) • A 100% bony union rate was obtained 12 months after PLIF with only local bone ( spine 2003 Miura Y) • A surgical technique of PLIF, with use of posterior elements cut into small corticocancellous chips measuring 2-4 mm as graft materal, has distinct advantages. (Clin Orthop Relat Res. 1985 Simmons JW)
PLIF without screw • To restore stability with no additional instrumentation, the cages must provide sufficent distraction of the vertebrae and adequate tension in the annulus ( Spine 2000 Goh JC ) • PLIF without PLF had advantages of the elimination of donner site pain, shorter operating time, and less blood loss. (Spine 2006 Kim KT MD)
PLIF with screw • Performing PLIF using stand-alone metallic cages, especially after total resection of the facet joints, is not advocated unless supplimental instrumentation is utilized. (Spine 2006 Cassinelli EH) • The combination of cages with dorsal instrumentation achieves a more precise realignment and has a lower rate of cage-associated complications ( Z orthopIhreGrenzgeb 2003 Diedrich O)
Cage migration • The rates of cage migration in patient with no posterior instrumentation was significantly higher compared with that rate in those with posterior instrumentation ( 16.7 %vs 0%) (Spine 2005 Chen, Liang MD) • Factors of cage migration – lack of posterior instrumentation and total facectectomy. (Spine 2005 Chen, Liang MD) • An Interbody fusion of lumbar segmental instability should be combined with pedicular instrumentation( Z orthopIhreGrenzgeb 2003 Diedrich O)
Cage가 빠지는 주된 원인이 Screw를 하지 않아서 라고 생각하십니까?
PLIF cage alone ( N=768, 1998-2006) • Retropulsion : 5 cases ( 0.6 %) Retry PLIF Cage alone, not screw • Pseudoarthrosis: 2 cases PSF and intertransverse fusion • Wound infection : 3 cases irrigation & resutured within 1 weeks not cage removal • No neurologic deficit
POD # 9days, Lt leg pain 23/M, PEEK cage F/U 1 yrs Varlock cage replacement
24/M, Varlock cage (11mm) inserted midline, contact 13mm reinserted laterally and intercage center bone POD# 1weeks, # 2 weeks
47/F POD #1 weeks Varilift (11mm)cage Varian(13mm) cage reinsertion F/U 3 yr flexion
Cause of retropulsion 0.6 % migration rate (5 / 768) reinsertion cage alone without screw fixation Cage insertion method >> combined screw • sufficent distraction of the vertebrae and adequate tension in the annulus ( Spine 2000 Goh JC ) • Proper preparation of the endplate prevents subsidence and increases fusion rate ( spine 2003, Oxland TR)
PLIF with cage alone is more effective method in specific cases One level fusion in multiple level instability Junction instability after screw fusion
1. Multiple level instability Screw보다 Junctionalinstability가 적다.
2. Junctional instability of screw fusion Screw후 Junctionalinstability에 cage alone 아주 효과적이다.
My history of CAGES Carbon CH PEEK Round VarlockVarlift TYM Varian
Upgrade expandible cage (Varian ) 56/F 3mo 6mo 5 yr early, long term F/U stable
Varian cage (Anchor) • Difinite expanded tripozoidal cage stabilize lordotic curvature • After inserted and expanded, bone chip filled ( clean, maximun amount chip) • Wide contact area and additional firm impacted bone chip area is spread pressure • Anterior angled shape cage insert easy and protect bony cortex
Varian cage (Anchor) • Simple one turn expansion (2-3mm) – strong hardware, long stable. Vs weak turn screw method • Select fitting cage, various size ( 9 -14mm, 2.4-2.7-3.0 cm) • Less subsidence, high fusion rate in long term F/U
Cage size AP diameter < 4 cm : 24 mm 4-5 cm : 27 mm > 5 cm : 30 mm 14mm 2.7cm Not fitting cage Fitting cage
Varian Cage (N=200 /2004.6-2006) • M:F 68:132 • Age 55.5 (14-76) • Degenerative spondylolisthesis 89 • Lyticspondylolisthesis 25 • Narrowoing & wedging anlgulation 86 • L2-3 4 • L3-4 34 • L4-5 156 • L5-S1 32 • Level 228 ( 2,3 level = 27 )
Varian Cage (N=200) • No cage related Cx ( migration, hardware Fx ) • Outcome (modified macnab classification) Excellent : 75 Good : 110 ( 93% ) Fair : 15 Poor : 0 • Radiologic fusion ( spine1991 Brantigan ) All cases radiologic fusion by flex/extension x-ray
F/U Radiography of Varian Cage B A A C Disc height (A+B)/C Segmental Total lordosis
Varian Cage (N=200) • Epidural anesthesia • Op time (1 level) : 112 minute • Bleeding loss : 191 cc • All local bone chip used • Center bone inserted between cages • Bed rest postop 5 day • TLSO brace postop 3 months
High grade spondylolisthesis with severe disc space narrowing
POD # 3mo 6months 45/F, two level PLIF F/U 5 yrs flex/ext F/U 2 yrs
51/F, severe lysis & listhesis POD#1 F/U 6mo F/U 2yr F/U 5 yrs flex/ext/AP
Conclusion of cage alone • Had many advantages of minimal invasive surgery • Could perform almost lumbar fusion surgeries • More effective fusion method in specific cases • Expandible Varian cage (anchor) is useful, good outcome, radiologic stable in long term F/U