Download
1 / 60
610 likes | 1.61k Views
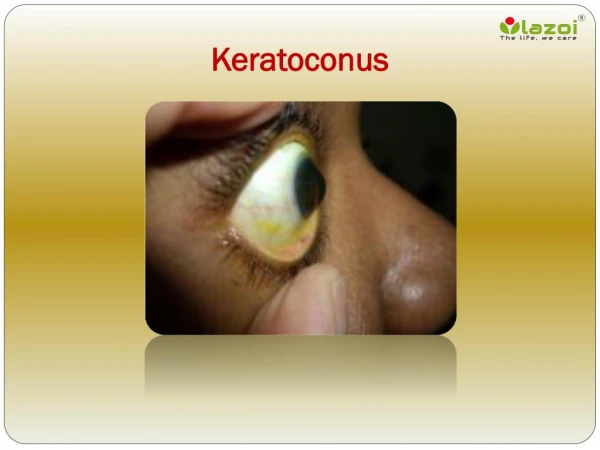
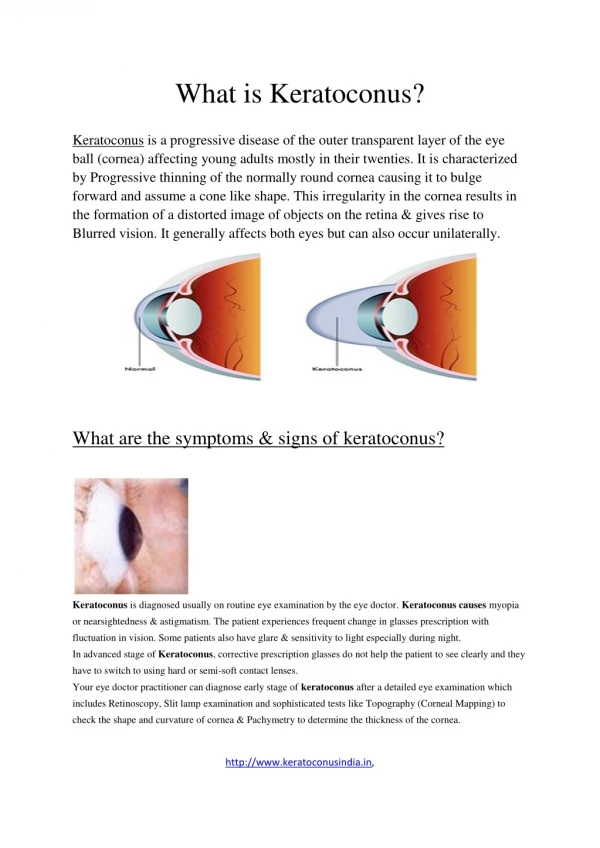
U pdate on Keratoconus Diagnosis and Treatment . Louise A. Sclafani, OD, FAAO Associate Professor University of Chicago. “Keratoconus is a clinical term to describe a condition in which the cornea assumes a conical shape because of thinning and protrusion”.

E N D
Update on Keratoconus Diagnosis and Treatment Louise A. Sclafani, OD, FAAO Associate Professor University of Chicago SCLAFANI
“Keratoconus is a clinical term to describe a condition in which the cornea assumes a conical shape because of thinning and protrusion” “Frustrated in my career because the cornea is so clear” Jay Krachmer, MD Professor, University of Minnesota SCLAFANI
Keratoconus History • Blurred vision • Distortion • Close WD • Photophobia • Monocular polyopia • Halos • Patient presents with frequent eyeglass changes SCLAFANI
Non-inflammatory 1/2000-5000 Central 2/3 AR/AD Inheritance Twin studies, chromo 5 Females =Males Presents initially at puberty & progression varies, stability in 30s 15 % need SX CLEK STUDY Observational study Multi center 1999 No race predilection 96% bilateral 13% FOHX QOL is worse than AREDS 3 VA, pain, mental,drive KCN HISTORY SCLAFANI
“Why don’t we see elderly patients with keratoconus” • Do they die younger NO • Do they not visit OD POSSIBLE • Have they CE/PKP POSSIBLE • Getting lenses from 1-800 • THEORY BY KRACHMER • The eye becomes more rigid as the patient ages and therefore the condition stabilizes SCLAFANI
ASSOCIATED SYSTEMIC CONDITIONS • Vernal KC • Atopic Dermatitis • Down’s Syndrome • Floppy Eyelid Syndrome • Mitral Valve Prolapse • Ehlers-Danlos Syndrome • Osteogenesis Imperfecta • Lawrence-Moon-Biedl Syndrome • Neurofibromatosis • Psuedoxanthoma Elasticum SCLAFANI
ETIOLOGY OF KCN • History of trauma that causes weakness • Recurrent trauma due to rubbing from • Blepharitis, CL/lids, 53% have atopic dx • Lieber’s- rubbing produces scotopsias • Pressure on corneal nerves is pleasing (right handed) • Inflammatory component !!! • Decrease proteinase inhibitors • Increase collagenase • Premature keratocytic apoptosis • Increase cytokine binding SCLAFANI
Basic Science Research • Christina Kenney, MD, PhD • KCN have higher # of mitochondrial DNA deletions that leads to decrease oxidative phosphorylation… increase H202 • Causes leakage, damages proteins, and results in oxidative stress • Leads to apoptosis, abnormal healing, inflammation. SCLAFANI
Aay, there’s the rub McMonnies CW. Mechanisms of Rubbing-Related Corneal trauma in Keratoconus. Cornea. 2009; 28:607-614 SCLAFANI
Basic Science Research • Yaron Rabinowitz, MD UCLA • KCN have suppressed Aquaporin 5 (AQP5) • AQP5 is the water transport gene that is responsible for cell migration and wound healing. • Quantitative PCR testing (epithelial cells) could diagnose this • IOVS April 2006 SCLAFANI
RESEARCH MAY INDICATE NEW THERAPIES • KCN is unlikely a single gene defect • Chromosome 5, 21 • Multiple genes in a common pathway • Those with the defect may develop KCN naturally or only if exposed to factors that induce oxidative stress: CL over-wear, UV, allergy or refractive surgery • TX: Anti-inflammatory, Anti-oxidant SCLAFANI
RETINOSCOPY • Scissors Reflex • Against motion that breaks apart • Represents multiple refractive powers within the optic zone SCLAFANI
KERATOCONUS-SLIT LAMP FINDINGS • FLEISCHER RING abrupt change in curvature 50% • VOGT’S STRIAE 1st Sign 65% • STROMAL THINNING • STROMAL SCARS • CLEK study showed • Steeper K 28% more scars • 43% of flat fits had scars • 26% of steep fits had scars • SWIRL-LIKE PATTERN • ENLARGED CORNEAL NERVES • ACUTE HYDROPS 5% SCLAFANI
EXTERNAL FINDINGS MUNSONS SIGN RIZZUTIS SIGN SCLAFANI
Keratoconus- Keratometry • Initially, mires get small and then there is a lack of parallelism • Expand perimeters by use of +1.25 SPH and add 7 D to your reading • Steepening begins infero-temporally and progresses clockwise • TOPOGRAPHY- more sensitive • PLACIDO RINGS- get closer SCLAFANI
PLACIDO RING IMAGES • Rings that are closer together represent areas of steeper curvature • May indicate a tight suture applicable SCLAFANI
Various Maps AXIAL Distance to reference point, not curves More global:excludes extremes Used for RGP fits: like K’s Sphere biased AKA: Sagittal=Color=Default TANGENTIAL Local or true curvature Best for shape analysis: disease Peripheral curve biased More detailed AKA: Instantaneous=True=Local SCLAFANI
ELEVATION (FLOAT) MAPS Predicts the relative elevation or depression of the cornea (in mm) using a computer generated BEST FIT SPHERE as a reference and fit at the steepest point SCLAFANI
ELEVATION MAPS PREDICT Na-FL PATTERN + VALUES- warm colors points higher than sphere = elevation Areas of bearing or touch - VALUES- cool colors points lower than sphere = depression Areas of pooling SCLAFANI
PELLUCID MARGINAL Tear meniscus can creates pseudo-PMD SCLAFANI
PMD vs. KCN SCLAFANI
PSEUDOKERATOCONUS • Corneal warpage topography can mimic KC • Repeat topography must be performed and a measurable change would indicate pseudo-KC • Evaluation of elevation maps at steep zone: • Predicts the elevation or depression of the cornea if the best fit sphere was on cornea SCLAFANI
POSTERIOR KERATOCONUS SCLAFANI
KCN Effects on Vision • Tim McMahon, OD • 60% reduction in VA is due to curvature, not just high cylinder • RGP corrects cylinder however HOA remain • COMA • May consider reverse geometry CLS • Reduced low contrast VA • Reads chart slower SCLAFANI
COMA Z31 • Similar to SA except that it concerns off axis peripheral rays that cause a comet-shaped image deformity to non-axial portions of the image. • Minimal • Post refractive surgery “Potato chip” due to flap hinge and shows the most dynamic change. SCLAFANI
Refractive Surgery • Corneal laser refractive surgery: pre-op, enhancement options • Phakic IOLs • Corneal refractive implants: Intacs • Anterior Segment Imaging and Surgery • Corneal Imaging and Measurement • Iris Imaging and Evaluation • Trauma Assessment SCLAFANI
Visante ApplicationsAnterior Segment Imaging and Surgery Corneal Imaging and Measurement • imaging and evaluation of corneal pathologies • penetrating keratoplasty • lamellar keratoplasty • endothelial keratoplasty • keratoconus imaging and assessment • anterior segment imaging through opaque corneas SCLAFANI
Terrien‘s Marginal Degeneration SCLAFANI image courtesy of Dr. M. Packer
Evolution of KCN: Ectasia to Hydrops SCLAFANI image courtesy of Prof. G. Baikoff
KCN/Open Angle (ML) SCLAFANI
KCN- Thinning (ML) SCLAFANI
Indications for Intra-Limbal Lenses • KCN RGP dropouts • Pellucid Marginal • Post-PKP • Astigmatic corneas • SCL failures: due to neovascularization or poor visual acuity. SCLAFANI
Corneo- Scleral 12.9 mm- 13.5 mm Semi- Scleral 13.6 mm- 14.9 mm Mini- Scleral 15.0 mm-18.0 mm Scleral Bearing, minimum corneal clearance Full Scleral 18.1 mm- > 24+ mm Scleral Bearing, maximum corneal clearance Dyna Intralimbal (Lens Dynamics) Macrolens (C&H) Jupiter (Innovations in Sight) GBL (Con-Cise) Large Diameter Lenses Robert Breece, OD SCLAFANI
Intra-Limbal Fitting • BC is Flatter than expected • K @ 4-5mm temporal vs. • Average Mid K +.2mm • Goal • Light feather touch • .2mm < corneal diameter (11.3 OAD) • .1-.2 mm movement • .2mm edge clearance • Menicon Z or Extreme • Unique ph or Claris SCLAFANI
SOFT LENS OPTIONS FOR KERATOCONUS • Soft Spheres • Soft Torics • X-cel Flexlens Tricurve • Basecurve 6.0 - 9.9 Diameter 10.0-15.0 • Center Thickness .45 dK 13.2 • Continental, Gelflex USA, Ocu-Ease (Ocuflex K) SCLAFANI
Benz 5x material,Glycerol Methacrylate Less dehydration, flexure,better optics Fit the normal peripheral cornea & sclera like standard SCL. The central posterior curve provides sagittal depth to touch POSTERIOR: Steep central curve, flatter paracentral peripheral curve all aspheric ANTERIOR: Central optical surface that quickly tapers to maximize 02 Low riding More movement SUPER NOVA HydroKone™ Innovations in Sight SCLAFANI
Innovations in Sight • SUPER NOVA HydroKone™Base Curves: 4.1 to 9.3 (5.3-8.5)Diameters: 12.0 to 17.0 (14.8) Paracentral: 8.0-9.2 (8.6) Sphere: +50.00 to -75.00Cylinder: -0.25 to -50.00Axis: 1 to 180 in 1 degree steps Mean K + 1mm Do not use H2O2 due to thickness EXPECT MORE MOVEMENT SCLAFANI
SynergEyes™A High Dk Hybrid Non-Ionic 27% water Hydrogel Skirt Paragon HDS 100® Rigid Center • Material • Paragon HDS 100 GP Center • 27% Water Non Ionic Skirt (Group I) • Design • 14.5 mm over all diameter • 8.4 mm rigid center • 7.8 mm optic zone • 2-4skirt radii choices for each base curve radius • Skirt thickness consistent across full power range • Engineered edge • HyperBond™ junction technology 8.4mm 14.5mm
SynergEyes KC Prolate ellipsoid base curve Spherical Skirt begins at 9.0 mm diameter 3 skirt curve options for fitting flexibility FDA Clearance December 2005 SCLAFANI
SynergEyes Fitting Lens Movement • .2mm to .3mm movement with blink • Slight lag in upward gaze • Free of scleral impingement • Free to move on “push up” • Free of “edge fluting” SCLAFANI
The Fitting Tips • Never prescribe Flatter than Flat K • Counter-intuitive: Corneas flatter than 44.25D and larger than 12.0 mm: Steeper Skirt Corneas Steeper 44.25D and smaller than 11.5 mm: Flatter skirt SCLAFANI
Identical Apical Radius with Different HVID = different sagittal depth 12.0 mm 3.60 2.96 11.0 mm
UPDATES FOR SYNERGEYES Proprietary materials that has a SiHy skirt and higher Dk GP The GP will have less flexure, will likely discontinue the enhanced profile To reduce peripheral crimping, the skirt curves will be multicurve: bi or aspheric CLEAR KONE : Additional KC lens for more ectopic or decentered peaks with reverse geometry to eliminate steep BC SCLAFANI
Vault the cornea yet aligns closer to cornea allowing lower powers Reverse geometry at skirt to allow more tear flow, easier removal SCLAFANI
TIPS ON PIGGYBACKS • SCL protects from RGP or environment • Reduces epithelial damage due to touch • Protects from apical nodules • Concurrent EBMD • High DK, easily replaced= SiHi • Soft Modulus molds to highly toric/steep K • +SCL to flatten the RGP • - SCL to steepen the RGP fit SCLAFANI
Intra-Stromal Rings • Ring segments are placed into peripheral corneal channels outside the visual axis to correct low to moderate myopia by flattening the cornea without cutting or removing tissue form the central optical zone • FDA approval of Intacs in 1999 for low/mod myopia. • Recently approved for keratoconus in US July 2004 Principle benefit: delay or eliminate corneal graft • Reversible/Removable SCLAFANI
Intacs Studies • By Wachler and et al. • 74 keratoconus eyes has insertion of intacs with F/U of 9 months • 45% gain ≥ 2 lines BCVA (worst pre-opt) • 51% had no effective changes • 4% loss ≥ 2 lines of BCVA SCLAFANI
Single intrastromal corneal implant favored for paracentral cones • Colin Chan, MD and Boxer Wachler,MD • Compared 20 eyes (double) vs. 17 (single) • Single used .25mm segment/ Double .25&.35 • All had paracentral/peripheral cones • Significantly better outcomes in change in cylinder, K values, UBVA, BCVA • Single 2-3 line gain, Double 1 line gain SCLAFANI
Complications of Intacs for KCN • Undercorrection • Overcorrection • Neovascularization toward the Incision • Migration of One segment toward the Wound • Extrusion • Stromal deposit • Flap wrinkling (intracorneal inlays) • Epithelial ingrowth • Residual refractive error • Complication rate ranges from 5-30% SCLAFANI