Download
1 / 45
470 likes | 604 Views
Aphasia Test 4. YOU WILL TOTALLY KICK ASS ON THIS TEST!!. Behaviors of Left Neglect. Excessive use of R Margin Perseverative- strokes in writing Safety Issues- hand in spokes of wheelchair Appear hemiplegic- looks like they are paralyzed. Can’t use leg or arm

E N D
Aphasia Test 4 YOU WILL TOTALLY KICK ASS ON THIS TEST!!
Behaviors of Left Neglect • Excessive use of R Margin • Perseverative- strokes in writing • Safety Issues- hand in spokes of wheelchair • Appear hemiplegic- looks like they are paralyzed. Can’t use leg or arm • Appear disinterested/unmotivated- won’t smile at you or laugh at your jokes. • Do not complain of disorder.
Neglect • Attention Disorder • Affects recovery • Duration Unknown • Mild to severe- spectrum mild (if you help them attend to neglected area, they’ll acknowledge it) to severe (won’t eat food on right side of plate). • Fractionation (occurs in multiple modalities)- olfactory, auditory info- we only work on comm. though- reading & writing.
Assessment • Informal observation- as soon as you walk in room- only looking to right. • Formal testing- very preliminary, not in depth • Tests of extinction (both sides of body)- testing sensation, for ex. Which finger am I touching? etc. • Line Dissection- draw a straight line, divide paper in half. Line will probably be over to the right. • Cancellation- if you see “A” cross it out. Make x’s out of target etc.
Assessment • Drawings - ask patient to draw semmetrical items. Draw a person, a flower, a clock etc. • Reading- (read ½ or less of text) read endings of sentences. Confabulation is good. • Writing- omit letters, forget to cross “t”, dot “i”. Perseveration, when you ask patient to write, they will write on top of their old writing.
Neglect • Subjective (point of view)- driven by patient. • Viewer centered- depends on the position of patient (turn in wheel chair). The most important for severe neglect. • Environment centered- more cognitive, there is another side to the door. • Object Centered (different perspectives) looking at objects at different perspectives.
Neglect • Other Modalities: • Auditory- but they can understand you. For some sounds though there is neglect. • Tactile- tests of extinction. • Olfactory- even if there is 1 olf. Bulb neglect, you can still smell w/ other nostril. • Motor- Affects contralateral movement. Client will act like hemiparesis. • Directional hypokinesia (moving limbs to contralateral space) Affects dressing, applying make-up. Seems like a strangers limb, someone else stole their shoes. Etc.
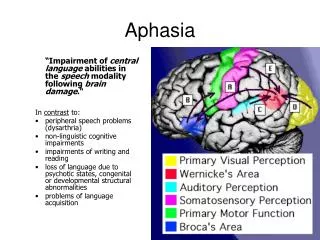
Areas of Damage for L Neglect • R MCA- middle cerebral artery • R Frontal Parietal Lesions • R Thalamus • R Basal Ganglia • R Hemisphere= less localization, more holistic
Theories of L Neglect • Representational- disruption of internal representation of space. How I see the flower. I can tell you what the flower and clock look like but can’t draw it. • Attention- • When cued, neglect is reduced. • Orienting bias- RH attends to R + L sides; LH attends to R- more specific. • Don’t see right neglect as often
Therapy for L Neglect • Bring awareness & attention to L side. • Severe deficits (tactile cue) • Physical Movement (wheel chair) • Moderate deficits (cue to neglected side) – have them feel around the plate , TV or book. • Mild deficits (teach to self cue) • I’m gonna have you highlight all the words on the left side of the page
Attention- Heirarchy • Arousal- eye contact (keeping eyes closed in bed). • Sustained Attention- attending to one thing for a prolonged period of time. • Put a cold washcloth on their face. • Selective Attention- knowing what is the most important task to focus on. • Divided Attention (multi-task)- completing multiple tasks at the same time. More for mildly impaired. • Treatment- task completion- • if they complete task, they can attend to it. If working on neglect, do task that addresess the area of neglect.
Goals for Left Neglect • 1. client will draw symmetrical items with 100% accuracy with tactile & visual cues. • 2. Client will turn to the left (look to the left) and/or describe items shown with 100% accuracy with tactile, visual and verbal cues. • Mild—look to the left with 100%, highlight written text on the left side. • If goal is to have a conversation, they can have a conversation for 5 minutes, attn OK.
Prosody • Melodic contour rhythm of speech. • Conveys meaning: • Emotional content • State of speaker- how is the speaker feeling? • Speaker’s attitude toward listener- sarcastic • RHD- monotone or euphoric • Linguistic effects- stress & syllable duration. Ex.- “green house”- spondee word. • Nonlinguistic (emotion, humor, formality) types of prosody.
Prosody cont.. • Pitch is vulnerable in RHBD (its affected) • Language can be intact, but prosody impaired. • Can cause divorce. • Emotional prosody most impaired. • Difficulty producing & comprehending emotions** • Facial expressions • Content of story- might not understand emotion of story. • Tx- patients need to identify their own emotions and others..
Emotional Prosody • Difficulty matching to emotion (pictures of sad, happy etc) • Monotone (no prosodic features)- for mild populations. • Prosodic contours- draw on paper where the stress should be. Ex. Yesterday was what? • Reliance on semantic info instead of prosody. Must be up front and literal. • Difficulty understanding sarcasm
Linguistic Prosody • Difficulty with compound nouns vs. noun phrases. (ex- light house) • Minimal emphatic stress (ex- she wore that dress) • Can’t correct prosody- can always teach them to be louder on stressed words. • RH perceives linguistic & emotional prosody • LH contributes to linguistic prosody.
MORE PROSODY!!! • Severe L Neglect= severe prosody deficits. • Prosody comprehension- R Anterior & Posterior cortical lesions • Linguistic prosodic deficits- R Frontal, temporal & parietal lobes, caudate nucleus, internal capsule, thalamus. • -- neglect guides how severe rest of deficits are.
Prosodic exercise… • List 5 sentences that provoke emotion: • 1. You look beautiful. • 2. What’s wrong? • 3. I had an amazing day. • 4. How do you feel about healthcare reform? • 5. I feel like I’m gonna throw up. • 6. Will you marry me? • 7. This food is delicious! • 8. Are you serious?
Linguistic Deficits • Perform normal on aphasia tests (w/ assistance for L Neglect) • Problems: Convergent & Divergent thinking. • Convergent: clues to the big picture- don’t get humor. Ex. It is small, you sharpen it, it has lead, an eraser.. etc • Divergent- single concept to more concepts (more clues) ie. problems with humor. Can only think of one meaning per word. Ex- give me 3 reasons that you would move to a different city.
Linguistic Deficits • Words with dual meanings are difficult • RH (works slower than LH) RH adds the nuances to language • Important for single word processing • Less frequent meanings • Slower & Less selective than LH • LH • Strong semantic overlap (words w/ several meanings) • Highly selective • Rapid in selection
Linguistic Deficits • Problems with collective nouns (eg. Furniture) • Abstract categories (ex- liquids) really difficult • More L Neglect= worse linguistic deficits. • Problems with Generative naming. Ex FAS. Name words that begin with F, A, S.
Think of 3 items that are more abstract than 3 concrete Abstract Concrete Types of fish Fruits Vegetables Farm animals Types of music • Things that are soft • Things that are rectangular shaped • Things that smell bad • Things that make you happy • Things that turn you on
Affect vs. emotion • Affect- outward expression of emotion (flat affect- show no emotion, look bored) • Emotion- subjective mood, state; internal experiences. How the person is feeling is not being shown. • RH Dominance Theory: • Perception • Comprehension • Expression of emotion • Emotional lability- used to describe affect- means constant crying or euphoria. Affect is impaired
Problems • With facial expressions (comprehension & production) • Promotes social isolation • Can comprehend gestures & posture • Problems w/ verbal emotions (stories, conversation) • Better identifying emotion when interested in story (written text) • Reduced prosody for emotional memories.
Depression (DSMR-IV) • 30-60% of RHD • 2 or more of the following: • Poor appetite or over eating • Insomnia or hypersomnia • Low energy or fatigue • Low self esteem • Poor concentration or difficulty making decisions • Feelings of hopelessness
Depression and RHD • Organic effects- change in neurotransmitters- serotonin • Reactive effects- response to deficits • Refer to neuropsych • Ask them if they are sad or unhappy. If they are depressed refer out.
Delusions & Confusions • Agitated Confusion- will see w/ TBI, because they are forming new connections. • Incoherent thoughts- similar to jargon • Easily distractible • Restlessness • Violent outbursts • Can occur w/ RHD but rare • Anterior Frontal & temporal damage (prefrontal cortex and executive function
Misidentification syndromes (person, place, body parts) • Will see them confabulate, make things up. • Look at own body parts and not know whose they are. • Reduplicative Paramnesia (place & person) • Imposter- they think you are one • Bifrontal or RH frontal and/or parietal lesions • Korsakoff’s syndrome- totally confused and paranoid. • Lack of Thiamine • Prolonges alcoholism- etiology • Looks like Wrnicke’s aphasia, fluent, jargon, neologisms
Campgrass Syndrome • Imposters- family members, friends- get neuropsych • Psychiatric component • Prosopagnosia (agnosia- sensory disturbance, occur w/ tactile & visual senses) • Visual agnosia- inability to recognize faces • Bilateral posterior lesions • No recall of familiar face • Tx.- if they can recognize voices work on that.
Somatoparaphasia: • Misidentification of own body parts (crossing midline) • Confabulation- about whose body part it is. • L Neglect • RHD disrupts the feeling of being connected and united.
RCVA • Discourse Deficits • Communicative event • Info conveyed by speaker to listener(s) • Requires situations content • Not all RHD have discourse problems- • may be high functioning patient • Cognitive problems= discourse deficits. • Cognition affect communication. • L Neglect= discourse affected • Simple discourse is intact. • Right hemisphere good verbal output. Abstract words difficult.
Anomia Goal • During anomic episode client will use semantic description, embedding and sentence completion • Verbal cues (sentence completion)- “describe cup” • Semantic descriptors- describe the cup, tell me the color, tell me where you find it. • Visual- point to the handle etc. Word Map.
Aud Comp goal • Client will answer yes/no question with verbal cues • Cues: repeat question, provide key words- Name Jamie? • Visual- point to Jamie. • Tactile- put jamie’s hand on herself when asked “Are you Jamie?”
Goals Continued • Complex yes/no questions- • Do you cut the grass with an ax? • How can you make it easier? • Does it snow in July? Simplify to two words • Repeat the ques. • Gestures for snow, July. Show pictures • Aud comp- major goal- UNDERSTAND CONVERSATION!!!
Cognitive communication- organization is an issue. They have problems with attention, organization. • L= neglect affects discourse too. • TYPES OF DISCOURSE: • Procedural- perform an activity • Expository- single topic/1 speaker (for TBI everything is expository) • Conversation- between 1 or more speakers • Narrative- event or story. Most difficult because it requires organization and structure.
Problems: • Inferencing: • Individual clues missed (attn) • Irrelevant clues selected • No intergration of clues (ie. No big picture) • Dissassociation of clues to prior experience • Indirect requests (ex. Boy, it’s cold in here) • Sarcasm (ex graceful!) • Humor (problems with punchline)
More deficits • Misunderstanding gist if info (macrostructure) • Difficulty with implied meaning (inferencing) • Providing alternative meanings • Lack of referent usage (Sam- who is Sam?) • Lack of sensitivity to communication content (ie. Comm. knowledge with listener
Higher level language • Figurative Language (Raining cats and dogs) • Literal info is easier (ie. Reduce sarcasm) • Cognitive Deficits: • WM- short term • Attention (because of L neglect) • Organization • Problem solving • Executive Function- lack insight etc. • Speed of processing- a lot slower..
Pragmatic Deficits (Social Language) • Initiation • Roles & Purpose (ex- code switching) • Turntaking (verbose, tangential) • Poor eye contact- related to L neglect • Poor organization
Theory of Mind • Understanding internal mental state of others (requires inferencing) • Assists in interpretation of external behavior • Informs about motivation(s), emotional state & knowledge base.
Evaluation of RHB • Medical chart • Interview • Informal assessment • Formal testing: • Burns Brief Inventory (neuropathologies & RH) • MIRBI-2 (mini inventory of right brain inventory) • Rehab institute of Chicago Assessment • Review Findings
Areas of Assessment • Cognitive (exec function, attn) • Orientation- to person, place, time, event • L neglect- tests of extinction, writing etc. • Discourse- Convo. • Prosody- listen for lack of prosody • Affective disorder- outward signs of emotion (wont get it) • Higher language function- abstract language • Pragmatic abilities- give them some jokes
Screening • 20 minutes • Tell me where you are today • What kinds of problems have you noticed? • What are your future plans? • What does your family/friends think about your plans? • What are you going to do today? • What kinds of people have you seen here?
Screening cont… • Picture: humor or inferencing • Emotion • Affect • Prosody • Higher lang function • L neglect
L neglect Screening • Cancellation task- make x’s out of paper. • Symmetrical drawing- clock, flower, person • Line Bisection- draw a line, divide it in half • Tests of extinction- touch hands or both hands • Reading/Writing- everything presented at midline