Download
1 / 68
690 likes | 1.07k Views
FISIOPATOLOGÍA (BCM II). Clase 8: Úlcera péptica. Dr. Michel Baró Aliste. “No acid, No ulcer” (Schwartz). No H. pylori, no ulcer? Yes acid, worse ulcer?. Hidrofobicidad de la mucosa Capa de mucus Producción local de bicarbonato Tight junctions Prostaglandina E2

E N D
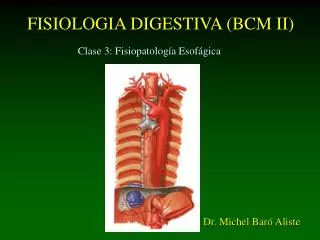
FISIOPATOLOGÍA (BCM II) Clase 8: Úlcera péptica Dr. Michel Baró Aliste
“No acid, No ulcer” (Schwartz) • No H. pylori, no ulcer? • Yes acid, worse ulcer?
Hidrofobicidad de la mucosa Capa de mucus Producción local de bicarbonato Tight junctions Prostaglandina E2 Flujo sanguíneo epitelial Recambio epitelial Inmunoglobulina A Epidermal Growth factor Transf. Growth factor alfa Acidez luminal, pepsina Substancias tóxicas (OH, AINES) Tabaco Helicobacter pylori Isquemia Factores agresores Factores Protectores
FISIOPATOLOGÍA Factores protectores
HCl injected through a column of mucin solution (a) Solución acuosa Efecto protector de la mucina
HCl injected through a column of mucin solution (b) Efecto protector de la capa de mucus
Proximal duodenal bicarbonate output was measured (a) Proximal
Proximal duodenal bicarbonate output was measured (b) Distal
Proximal duodenal mucosal bicarbonate secretion was assessed (a) Acetazolamida
Proximal duodenal mucosal bicarbonate secretion was assessed (b)
Afferent nerve-mediated gastric mucosal hyperemia (a) CGRP=calcitonin gene-related polipeptide
FISIOPATOLOGÍA Factores agresores: Hipersecreción ácida Helicobacter pylori AINESs Otros factores
Hipersecreción ácida gástrica • Hipergastrinemia dependiente de H. Pylori • Hiper-secreción independiente de H.P. ( tono vagal) • Masa parietal intacta (gastritis tipo B)
Gastric acid secretion comparison (a) 7,1 mmol/h 3,3 mmul/h
The Nobel Prize in Physiology or Medicine 2005 "for their discovery of the bacterium Helicobacter pylori and its role in gastritis and peptic ulcer disease" Barry J. Marshall J. Robin Warren NHMRC Helicobacter pylori Research Laboratory, QEII Medical Centre; University of Western Australia Nedlands, Australia b. 1951 Perth, Australia b. 1937
Tests for diagnosis of Helicobacter pylori can be categorized Inmunoensayo en deposiciones: HpSA
Association of Helicobacter pylori with gastrointestinal disease
Patogenia de la úlcera por H. pylori • Aumento de la secreción ácida • Metaplasia gástrica del duodeno • Respuesta inmune • Mecanismos de defensa
1-Hipersecreción ácida • H.P. Induce aumento de liberación de gastrina • Efecto trófico en cel. Parietales y ECL • Estímulo cel. Parietales, vía histamina • H.P. Disminuye concentración de somatostatina
2-Metaplasia gástrica del duodeno • Presencia de epitelio gástrico en la primera porción del duodeno. • Aparece en respuesta a la exposición ácida pH <2,5 • Secreción de bicarbonato disminuida por H.P. • Focos metaplásicos permiten colonización por H.P.
2-Metaplasia gástrica del duodeno • Cepas Cag A(+) más común en ulcerosos duodenales que en infectados asintomáticos (80% versus 30%) • H.P. Debilita la mucosa con metaplasia gástrica • RR de úlcera duodenal en metaplasia gástrica =5 • RR de úlcera en mataplasia gástrica + H.P. =50
3-Respuesta inmune • H.P. No invasor, pero induce gran respuesta inflamatoria • Cepas VacA y CagA poseen mayor patogenicidad • Aumenta IL-1, IL-2, alfa-TNF, IL-8 • IL-8 activa los neutrófilos (Cepas Cag E) • Activación linfocitos B, con producción de IgG e IgA • Estimulación prolongada de linfocitos B por activación de linfocitos T puede desencadenar hiperplasia folicular, linfoma MALT
4-Alteración de factores de defensa de la mucosa • Epidermal Growth factor (EGF) y Transforming growth factor-alfa (TGF alfa) son potentes inhibidores de la secreción gástrica y promotores del crecimiento y protección de la mucosa. Post-erradicación de H. pylori. • Bicarbonato del duodeno proximal en pacientes con U.D. • Proteasas de H.P. degradan glicoproteínas del mucus