Download
1 / 19
200 likes | 237 Views
Reverse Total Shoulder Arthroplasty (Reverse TSA). Heidi Church, SPTA Fall Internship 2012 Salt Lake Orthopaedic Clinic 1160 East 3900 South, Suite 4050 Salt Lake City, UT 84124. Facts.

E N D
Reverse Total Shoulder Arthroplasty (Reverse TSA) • Heidi Church, SPTA • Fall Internship 2012 • Salt Lake Orthopaedic Clinic • 1160 East 3900 South, Suite 4050 • Salt Lake City, UT 84124
Facts • Epidemiology - in United States there are ~53,000 total shoulder arthroplasties per year compared to >900,000 total hip & total knee arthroplasties per year (9) • Indications for a Reverse TSA - ~80% of patients needing a reverse TSA have glenohumeral (GH) joint degradation and an inefficient rotator cuff, while ~18% have a good GH joint, an irreparable rotator cuff injury, and are >70 years of age. The remaining 2% have a failed TSA • 90% to 95% of patients with osteoarthritis, requiring a TSA, have their rotator cuff intact. That means 5%-10% have a deficient rotator cuff. (10)
Glenohumeral Joint • Articular surface: inclined 130˚-150˚to the shaft of the humerus, and retroverted 20˚-30˚ (10)
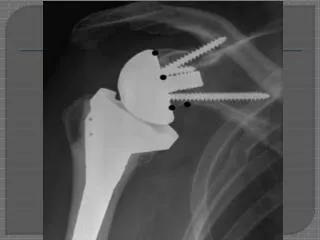
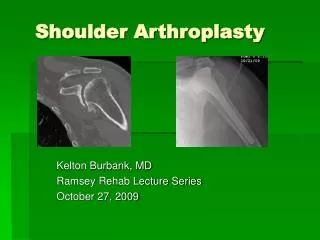
Anatomy of shoulder after Reverse TSA • coracoid process of scapula • acromion • humerus • prosthetic ball • prosthetic socket • scapula
Biomechanics of Reverse TSA • glenoid center line - “In a normal glenoid, the center line represents a line perpendicular to the articular surface of the glenoid and directed, on average, approximately 10° posterior (retroverted) to the plane of the scapula (Fig. 5A–B). The center line serves as the pillar under which the humeral head rests; glenohumeral and scapulothoracic motion are coupled to maintain the center line beneath the humeral head throughout the shoulder’s ROM. (4) In cases of severe or eccentric glenoid wear, a stable baseplate fixation can only be achieved by placing the component along the alternate glenoid center line (Fig. 5C–D). This alternate center line is defined as a line aiming at the dense bone where the scapular spine meets the body of the scapula and is not necessarily perpendicular to the remaining glenoid face.”(4)
Forces on baseplate-bone junction glenoid position of prosthetic head
Deltoid Muscle • = axis of rotation • When the axis of rotation is moved laterally, the deltoid muscle’s movement becomes one of rotation.
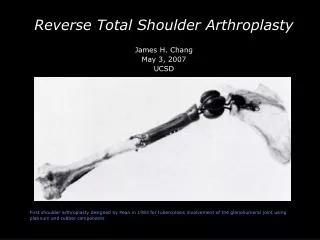
History of TSA/Reverse TSA (3) • 1893 - first prosthetic shoulder arthroplasty - performed by French surgeon Jules Emile Péan • 1955 - proximal humeral arthroplasty used to repair fractures - Neer • 1970’s - surgeons face the challenge of developing a satisfactory prosthesis that balances joint stability and ROM. Reversed normal anatomy designs for TSA • 1972 - divergent threaded peg glenoid component - Leeds • 1973 - Single central screw - Kessel. Hydroxyapatite coated large central screw (screw thread diameter increased), center of rotation moved medially and distally - Bayley-Walker • 1973-1981 - rotator cuff and constraint in total shoulder arthroplasty - Neer designs three implants, Mark I, II, III • 1975 - emphasis on enlarged ball-and-socket to increase glenohumeral motion and increase deltoid lever arm - Fenlin • 1978 - floating fulcrum, small glenosphere articulating with larger intermediate polyethylene cup, to allow supraphysiologic motion. - Buechel • 1985-1994 - Grammont’s system introduced, four key features: 1) prosthesis must be inherently stable; 2) weightbearing part must be convex, and supported part must be concave; 3) center of sphere must be at or within glenoid neck; 4) center of rotation must be medialized and distalized. 1991 - Grammont’s second generation design changed the glenosphere from 2/3 of a sphere to 1/2 a sphere, and the baseplate included a central press-fit peg and two divergent 3.5-mm screws. 1994 - Grammont’s third variation changes directed toward the humeral component.
Rehabilitation for the Reverse TSA(6) • Early Passive Motion (0-4 weeks) - wear sling to week 3, passive/self-passive (pulley) ROM in forward flexion(FF) up to 90˚ and external rotation(ER) up to 45˚ • Active Assistive Motion (4-6 weeks) - self-passive (pulley) ROM in FF up to 120˚, ER to 45˚ • Active Motion (6-8 weeks) - active assistive ROM in FF up to 145˚ and ER up to 45˚ • Full Stretch (8-10 weeks) - full stretch in FF and ER, increase isometric muscle contraction, and add small amounts of weight, as tolerated • Strengthening (10-12 weeks) - increase weights and build deltoid muscle strength
1} 2} 4} 3} Early Passive Motion (0-4 weeks) • 1}Passive manual ROM forward flexion-90˚ • 2}Passive manual ROM external rotation to 45˚ • 3}Self-passive, with pulley, forward flexion to 90˚ • 4}Self-passive, with pulley, external rotation to 45˚
2} 1} Active Assistive Motion (4-6 weeks) • 1} Active Assistive ROM, with pulley, forward flexion to 120˚ • 2} Active Assistive ROM, with pulley, external rotation to 45˚ • 3} Gripping exercises
1} 3} 2} Active Motion (6-8 weeks) • 1}Pulley - forward flexion, external rotation • 2}Ladder - forward flexion • 3}Dowel supine - forward flexion
1} 2} 4} 3} Full Stretch(8-10 weeks) • 1}Internal rotation stretch with belt, horizontal/vertical • 2}Supine horizontal adduction stretch • 3}Ladder - forward flexion with isometric hold off ladder • 4}Dowel supine - forward flexion with weight as tolerated
1} 2} 3} Strengthening(weeks 10-12) • 1}Deltoid muscle strengthening - forward flexion • 2}Deltoid muscle strengthening - abduction • 3}Internal rotation strengthening
Goals • Decrease pain • Improve range of motion • Improve strength • Improve functional ability
Complications • Infection - any infection in the body can spread to the prosthesis. • incision site • deep around prosthesis • minor - treated with antibiotics • major - may require surgery and removal of prosthesis • Prosthesis problems • wear • components loosen • dislocation • Nerve injury
Prognosis • SLOC case study - pain < 1/10, SPADI < 25%, percent of function 80% • Revision rates of RTSA 4.2% - 13% • Instability rate of 2.8% • RTSA for cuff tear arthropathy “results in major improvements” (7)
References • 1) Acta Orthopaedica, Dec2010, Vol. 81 Issue 6, p719-726, 8p, 9 Diagrams, 1 Graph, Diagram; found on p720 • 2) Nolan B, Ankerson E, Wiater J. Reverse Total Shoulder Arthroplasty Improves Function in Cuff Tear Arthropathy. Clinical Orthopaedics & Related Research [serial online]. September 2011;469(9):2476-2482. Available from: Academic Search Premier, Ipswich, MA. • 3) A History of Reverse Total Shoulder Arthroplasty, Evan L. Flatow, Alicia K. Harrison, Clin Orthop Relat Res. 2011 September; 469(9): 2432–2439. Published online 2011 January 7. doi: 10.1007/s11999-010-1733-6, PMCID: PMC3148354 • 4) How Reverse Shoulder Arthroplasty Works, Matthew Walker, Jordan Brooks, Matthew Willis, Mark Frankle, Clin Orthop Relat Res. 2011 September; 469(9): 2440–2451. Published online 2011 April 12. doi: 10.1007/s11999-011-1892-0, PMCID: PMC3148368 • 5) http://jimmysmithtraining.com/six-pack-diet/good-hurt-bad-hurt • 6) Salt Lake Orthopaedic Clinic protocol for Reverse Total Shoulder Arthroplasty • 7) Reverse Total Shoulder Arthroplasty Improves Function in Cuff Tear Arthropathy. Betsy M. Nolan, Elizabeth Ankerson, J. Michael Wiater. Clin Orthop Relat Res. 2011 September; 469(9): 2476–2482. Published online 2010 November 30. doi: 10.1007/s11999-010-1683-z. PMCID: PMC3148381 • 8) http://www.umm.edu/orthopaedic/rsr.htm • 9) http://orthoinfo.aaos.org/topic.cfm?topic=A00094 • 10) Physical Therapy of the Shoulder, fourth edition, edited by Robert A. Donatelli • 11) http://my.clevelandclinic.org/services/shoulder_replacement/hic_total_shoulder_joint_replacement.aspx