Download
1 / 43
430 likes | 622 Views
Rate in beats/min = 60/interval between two beats in seconds A handy shortcut is: Heart rate (beats/min) = 1500/R-R interval (mm). 1500/20 = 75 b/min.

E N D
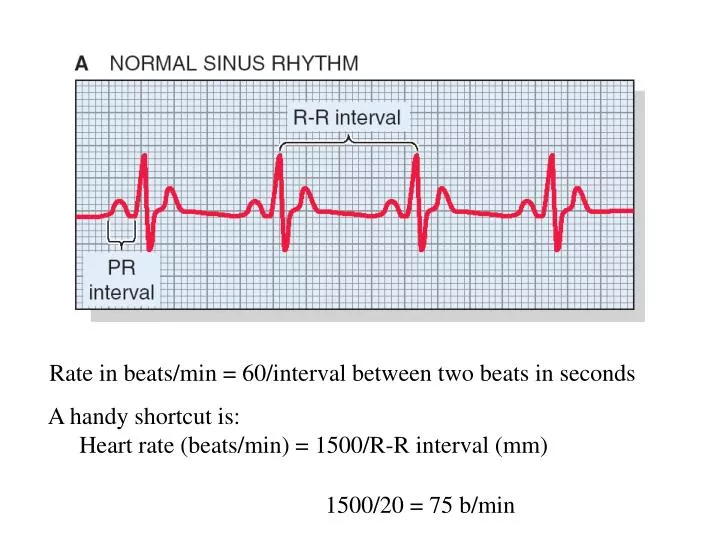
Rate in beats/min = 60/interval between two beats in seconds A handy shortcut is: Heart rate (beats/min) = 1500/R-R interval (mm) 1500/20 = 75 b/min
Heart block Heart block results when conduction between the atria and ventricles is altered. This often occurs at the AV node which has a low safety factor.
8 x .04 = .32 sec First degree - prolonged PR interval only. The normal PR interval is 0.12 to 0.21 seconds. A PR interval >0.21 would be classified as first degree block. The injury is above the His bundle because His conduction is very fast even when injured.
Second degree - some P waves are not followed by QRS. Often has a regular sequence, i.e., 2:1 or 3:2. The first number is the number of P waves present and the second is the number of QRS’s. What is this?
Mobitz I (Wenckebach) the PR progressively lengthens with one P wave for every QRS until a beat is dropped. Usually this block occurs above His bundle. This is common in coronary patients and is caused by increased vagal tone and usually eventually disappears with no problems
Mobitz II 2nd degree heart block missed beats with no change in P-R It is a dangerous arrhythmia because the heart may suddenly start beating very slowly or even stop. The injury is below the AV node in the fast conducting His bundle where the pacemaker activity is very slow
Complete heart block. Since there is no conduction down the AV node pathway both atria and ventricles beat regularly but at different rates (ventricles always slower).
Slow ventricular rate Usually treated with pacemaker May be temporary or intermittent. Can be induced by drugs that cause increased vagotonia (e.g. neostigmine) or slow conduction in the AV node (e.g. beta blockers or calcium antagonists)
WPW: Normally conducting cardiac muscle bridges the gap between atria and ventricles. The accessory pathway activates the ventricle before normal activation via the AV node.
The PR interval is <0.12 sec Delta waves are usually present
If accessory pathway has short antegrade refractory period, it will cause the ventricle to beat dangerously fast if atrial fibrillation occurs. Ventricles pump very poorly at high heart rates. Can get retrograde conduction causing reentry and a tachycardia.
Normal sinus rhythm Sinus tachycardia Sinus bradycardia Sinus Tachycardia >100b/min 1. Normal P waves all followed by QRS 2. Normal or shortened PR interval 3. QRS and T vectors are normal 4. ST segments are normal 5. RR interval is regular but short <15mm 1500/15 = 100
Normal sinus rhythm Sinus tachycardia Sinus bradycardia Sinus Bradycardia <60b/min 1. P waves are present and all are followed by a QRS 2. Normal and constant PR interval 3. QRS and T vectors are normal 4. ST segments are normal 5. RR interval is regular but long >25mm 1500/ 25 = 60
Premature ventricular contraction (PVC) 1. Arises from ectopic focus in ventricles 2. Early QRS not preceded by a P wave (see fig 4) 3. Will usually have an unusual QRS shape a) odd vector b) prolonged QRS duration 4. A compensatory pause
Premature ventricular contraction (PVC) 5. The premature contraction occurs before the ventricle is completely filled and the contraction may be two weak to open the aortic valve. 6. The beat is not felt in the peripheral pulse and can be mistakenly thought to be a second degree block. 7. The following beat has an over-filled ventricle and is very strong (this is often perceived by the patient)
Multifocal PVCs. Two separate foci are originating PVC’s Irritable ventricle IF all PVCs are identical it is from only one ectopic site (Unifocal).
Premature atrial contraction (PAC) 1. Arises from an ectopic focus in the atria. 2. Will have an identifiable P wave but the shape of the P wave may be altered 3. May have a normal QRS 4. compensatory pause will be small or absent
The compensatory pause is lacking because the SA node was reset. The rhythm has been shifted. The QRS may be altered if some of the ventricle is still in its refractory period (the P wave is the key, not the shape of the QRS).
Electrical reentry can cause fibrillations and tachycardias.
Atrial fibrillation 1. Irregularly irregular 2. No P waves
The AV node acts to keep the ventricular rate low May be treated with drugs to depress AV conduction and slow the ventricular rhythm: Beta blockers, calcium channel blockers 8 beats in 6 seconds or 80 beats per minute
Common: will occur in about 1/3 of the population Lowers cardiac output if ventricular rate is high Not a life-threatening arrhythmia unless in WPW Stroke risk - anti coagulation may be indicated
Atrial flutter occurs when the atrium beats very rapidly rather than fibrillates. The AV note filters out most beats so the ventricle beats at a slower rate. Note the presence of multiple p waves between QRS complexes.
1500/9=166 Ventricular tachycardia (3 or more sequential beats) 1. Regularly occurring rapid rhythm originating from a regularly firing ventricular ectopic focus. 2. QRS morphology is usually like a PVC (depending on where the ectopic is located)
Because the cardiac output falls due to the fast rate it often produces (or worsens) myocardial ischemia which then makes ventricular fibrillation more likely
VF Ventricular fibrillation (VF) 1. Thought to be a reentrant excitation of the ventricles; premature impulse may arise during vulnerable period 2. Irregular baseline with no identifiable waves
3. No cardiac output. Usually the cause of "sudden death" 4. May be the result of ischemia, lightning strike, electrocution, chest trauma, or drugs 5. Requires CPR and electrical defibrillation. Patients do not spontaneously recover.
The defibrillator gives a strong electrical pulse of current across the chest so that all heart muscle cells are put into an action potential. A refractory period follows that usually breaks the conducted arrhythmia.
Control Norepi Q-T interval is rate- dependent and is an index of the duration of phase 2 in the ventricular AP
In long QT syndrome the QT interval is longer that the maximal normal value for that heart rate. Q-T 12 x 40 = 480 ms Rate 1500/15 = 100 b/min
Long QT syndrome • Prolonged duration of phase 2 causes an early afterdepolarization. That can trigger an early action potential causing a reentrant tachycardia • Patients may experience attacks of VT with torsades de pointes - a waxing and waning of the QRS morphology (as if circling around a point).
3. Long QT is induced by some drugs and can be due to genetic abnormalities in some potassium and calcium channels. At present 5 separate genetic defects have been identified which cause long QT
14 STEPS TO ASSURE A SUCCESSFUL READING AND UNDERSTANDING OF AN UNKNOWN ECG 1. Is the ventricular rhythm regular?2. Are there P waves?3. Is the atrial rhythm regular?4. Is there one P wave for each QRS?5. What are the atrial and ventricular rates?6. What is the P-R interval?7. Is the P-R interval constant?8. Are there extra or premature beats?9. What is the QRS duration?10. Does the QRS morphology indicate presence of a conduction defect? 11. What is the mean electrical QRS axis?12. What is the mean electrical P wave axis?13. Is there S-T segment deviation?14. Are there pathologic Q waves?