Download
1 / 34
340 likes | 548 Views
Case Based Learning Pharmacology . HSS 3101. Learning Objectives . To understand the anatomical, physiological, and pathological processes involved in cardiac emergencies. To understand the pharmacological and alternative treatment options available for cardiac emergencies.

E N D
Case Based Learning Pharmacology HSS 3101
Learning Objectives To understand the anatomical, physiological, and pathological processes involved in cardiac emergencies. To understand the pharmacological and alternative treatment options available for cardiac emergencies. To become familiar with the first aid approach involved in cardiac emergencies. To understand the social factors involved in the pathogenesis of various cardiac disorders that consequently result in cardiac emergencies.
Case Introduction A 53 year old man, Mr. David Smith, suddenly started having chest pain. His wife called the ambulance, and paramedics responded within 15 minutes of the onset of his chest pain. He was taken to the Ottawa Heart Institute at 2:12 am.
Pre-hospital care Discuss how paramedics differentiate between serious and benign chest pain. Discuss the various first aid measures that paramedics use if they suspect cardiac emergencies. What other important questions should paramedics ask Mr. Smith or his wife?
Paramedic Report 53 year old Caucasian male presented with acute onset, sharp sub-sternal chest pain that radiates to his neck. He describes the pain as “a ton of bricks” sitting on his chest. He describes the pain as 9/10 and has positive Levine’s sign. The pain is not responsive to 2 aspirin 325 mg PO and nitroglycerine 2.2mg sublingual. ECG shows hyper-acute T waves.
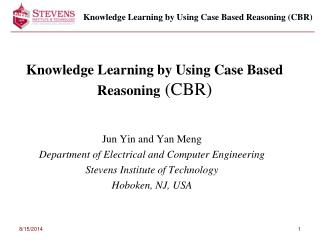
Paramedic Report Referred Pain
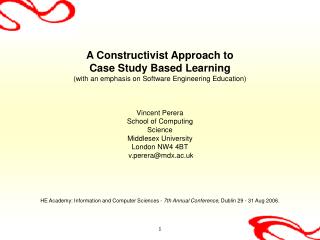
Paramedic Report Normal ECG
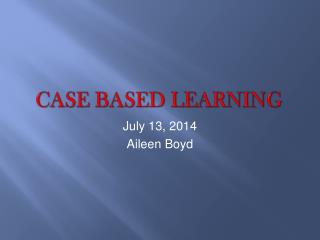
Paramedic Report Patient’s ECG
Paramedic Report • The patient is diaphoretic, pale, and anxious on exam. • Blood pressure is 145/90 • HR is 120, RR is 21 with dyspnea • Temperature is 38oC. • The patient is started on high flow oxygen and given 2 mg morphine sulfate. • Narrow your differential diagnosis and discuss the results paying attention to vitals and ECG results.
Emergency room CC: Acute substernal chest pain HPI: Mr. Smith suddenly woke up and realized he was having severe chest pain 9/10, his wife called 911, the patient denies severe exercise of sexual activity prior to onset.
History Medical Hx Mr. Smith has a of 2-y history of hypertension for which he has been taking HCTZ 25 mg/d (compliance?), Mr. Smith denies any history of hypercholesterolemia or diabetes. The patient’s father died of an MI (myocardial infarction) at age 54, and his brother underwent coronary artery bypass graft surgery 3 years ago at age 46. Not taking any medications other than HCTZ No known drug allergies
History continued Social Hx • Mr. Smith smokes two packs of cigarettes per day for 35 years, drinks alcohol moderately. • He’s married for 25 years and has three children. • He graduated from High School. • He attends church regularly. • Hobbies include woodworking and gardening. • He drinks one to two cups of coffee per day. • He denies exposure to environmental toxins. • He denies any financial problems but is concerned about how his illness will affect his income. • Mr. Smith is not physically active and is obese (BMI>30). • His sources of support are his wife, minister, and a sister who lives near the patient.
History discussion Construct a pedigree with the information given, how would you obtain more information. Discuss the cardiovascular risk factors. What will you be looking for in the physical examination?
Physical Examination • General: • Mr. Smith is a pleasant male lying comfortably supine in bed. He appears to be the stated age with a BMI of 32. • Vital Signs: • Temp 38.1°C orally • Respiration 23 • Heart rate (HR) 121 and regular • Blood pressure (BP) 142/93 left arm supine • Skin: • Tattoo left arm, otherwise no lesions
Physical examination • Eyes: • External structures normal, without lesions, PERRLA. • EOM intact. • Visual fields intact. • Benign fundoscopic exam. • Mouth: • Several dental fillings, otherwise normal dentition. • No lesions • Chest: • Symmetrical expansion. • Lung fields clear to percussion. • Breath sounds normal except end-inspiratory crackles heard at both bases that do not clear with coughing.
Physical examination • Heart: • No cardiac impulse visible. • Apical impulse palpable at the sixth intercostal space 2 cm lateral to the midclavicular line. • Normal S1, physiologically split S2. S4 heard at apex. • No murmurs, rub, or S3. • Abdomen: • Flat, no scars. Positive bowel sounds. • No bruits, no CVA tenderness. • No hepatomegaly or splenomegaly by palpation. • No tenderness or guarding. • No inguinal lymphadenopathy.
Physical examination • Peripheral Vascular: • Radial, ulnar, brachial, femoral, dorsalispedis, and posterior tibial pulses +2/4 bilaterally. Popliteal pulses nonpalpable. No femoral bruits • Neurologic: • Cranial nerves: I through XII intact. Motor: +5/5 upper and lower extremity, proximally and distally. Sensory intact to pinprick upper and lower extremities proximally and distally. • Respiratory: • Notes cough every morning and has produced 1 teaspoon of gray sputum for years. Denies hemoptysis or pleuritic chest pain. Last chest x-ray prior to today was 3 years ago.
Lab tests Which tests would you consider, why and what would you expect to see? What are the cost of these tests? How invasive are these test (prioritize) How is the sensitivity and specificity of these tests (compromised?) Are they affected by any other factors eg. diet, time of the day, muscle mass etc.
Variations of cardiac proteins in serum Hours of onset of problem
Lab results • Chemistry Profile: • Normal, except elevated CPK and Troponin • CBC: 6700 • WBC: 49 • Hct; HBG 16; 40 S, 5 B, 44 L, 5 M, 6 E • PT, PTT: Normal • What do these results indicate, what is your next step?
ECG ECG. HR 123, ST elevation V1 through V5.
Imaging studies R L Chest X-Ray: Cardiomegaly, otherwise clear
Diagnosis Myocardial Infarction
Assessment and Plan • Mr. Smith presented with a classic history for MI. The CPK, troponin and electrocardiogram support the diagnosis. Since he was taken to the hospital within 3 hrs of symptom onset he is a candidate for Thrombolytic therapy • Treatment regimen • ASA • Beta Blocker • Ace inhibitor • tPA • Statin
Pharmacological therapy Discuss the indication and contraindication for the various medications paying close attention to all aspects of Mr. smiths history. Discuss the pharmacokinetics and pharmocodynamics of the selected medications. Discuss the toxicity and the adverse effects of the medications and the potential for drug interaction.
Follow-up While in observation, Mr. Smith started having shortness of breath which was slightly improved when his bed was elevated to 45 degrees (orthopnea), he also had an episode of sudden night time attack of severe breathlessness. On examination, Mr. Smith had crackles heard initially in both lung bases and a displaced apex beat. ROS reveals no pitting peripheral edema, ascites, and hepatomegaly.
Lab Tests Formulate a new DDx list Explore the various ways to test your hypothesis. What laboratory tests would you consider and what would you expect What imaging studies would you consider
Lab results Troponin and CK was within normal limits Mr. Smith had elevated B-type natriuretic peptide EKG identifies left ventricular hypertrophy Other laboratory results were within normal limits Echocardiography revealed reduced ejection fraction.
Results Discuss what the imaging studies and laboratory values indicate. Why is this patient having this problem?
Treatment Pharmacological therapy Beta Blocker Ace inhibitor Angiotensin receptor blocker Cardiac glycosides Calcium channel blocker Antiplatlets Diuretics
Pharmacotherapy Name two medications within each class and how it can be used in heart failure Discuss the mechanism of action and pharmacokinetics of these medications Discuss the adverse effects, toxicity, side effects and potential for drug interactions Discuss the other methods that can be used in treating heart failure.
Follow up Mr. Smith’s condition continued to deteriorate at home for the next few days. He suffered a pulmonary embolism which led to cardiac arrest. He was rushed to hospital, but he was pronounced D.O.A.