Download
1 / 29
310 likes | 677 Views
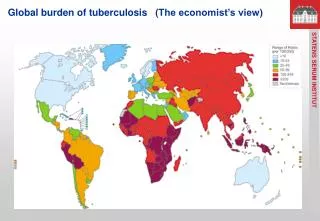
Global progress in tuberculosis vaccine development. Helen McShane The Jenner Institute University of Oxford. Global Plan to Stop TB: 2006 - 2015. Targets (from MDGs) > 70% with infectious TB will be diagnosed >85% of those will be cured By 2015, global prevalence of TB will be

E N D
Global progress in tuberculosis vaccine development Helen McShane The Jenner Institute University of Oxford
Global Plan to Stop TB: 2006 - 2015 Targets (from MDGs) > 70% with infectious TB will be diagnosed >85% of those will be cured By 2015, global prevalence of TB will be reduced to 50% of 1990 levels By 2050, global incidence will be <1/million population How? Use of current tools DOTS; DOTS-plus; DOTS expansion New tools New drugs New diagnostics New vaccines Total cost of plan: US$ 56 billion – US$ 31 billion funding gap
BCG Live attenuated Mycobacterium bovis First used in 1921 (per os) Efficacy: Good Disseminated TB and TB meningitis Leprosy Bad Lung disease Boosting (Rodrigues et al, Lancet 2005) Efficacy highly variable (0 – 80%)
Why is the efficacy of BCG so variable? Different strains of BCG Nutrition Exposure to environmental mycobacteria Masking (Black et al, 2002) Blocking (Brandt et al, 2002)
Other problems with BCG • Safety in immuno-suppressed • Contra-indicated in HIV-infected adults • Risk of disseminated BCG disease in HIV-infected infants • Change of WHO policy • Relative balance of risks
What do we know about protective immunity Essential: CD4+ T cells IFN γ TNF Probably important: CD8+ T cells γδ T cells CD-1 restricted T cells IL-17 Il-2 Probably not a major role B cells and antibodies
Design of an improved vaccine against TB • Include BCG in new regime • Needs to induce cellular immune response • 3 possible strategies: • Enhance BCG with a subunit vaccine • Protein + adjuvant • Viral vector • Replace BCG with improved BCG / attenuated M. tb • Enhance an improved BCG
Recombinant BCG strains rBCG-30 (UCLA/AERAS) First time in man February 2004 Not currently active ΔureC hly+(MPI Berlin / VPM) Phase I study in Berlin complete Phase I/IIa in South Africa ongoing Aeras 422: rBCG expressing Ag85A, B and Rv3407 Phase I study commenced in Q1 2011 Now withdrawn for safety reasons
Attenuated M.tb strains • Pho p-/- (Martin, Zaragosa) • Pantothenate auxotroph (Jacobs, HHMI) • IKE-PLUS (Sweeney et al, NM 2011)
Booster vaccines: MTB 72F / M72 • GSK • 32/39kDa antigens • AS01 adjuvant. • First time in man February 2004 • In Phase IIa in South Africa and The Gambia • Antigen-specific CD4+ T cell responses Von Eschen et al, 2009
Booster vaccines: SSI fusion proteins • Hybrid 1 (ESAT6/85B) • IC31 novel adjuvant • First time in man November 2005 • Confounds diagnostic tests • HyVac 4 (TB10.4/85B) • Phase I in Europe complete • Phase I/IIa in South Africa ongoing • Hybrid 56 (ESAT6/85B/Rv2660) • Phase I underway in South Africa Van Dissel et al, 2010
Booster vaccines: Aeras 402 • Ad35-85A,B,TB10,4 • Aeras/Crucell • First time in man Oct 2006 • Phase I/IIa study in South Africa complete • High antigen-specific CD8+ T cell responses • Phase IIb in infants underway • Abel et al, AJRCCM 2010
Modified vaccinia Ankara (MVA) Poxvirus No replication in mammalian tissues Good T cell boosting vector Excellent safety record M.tb antigen 85A Mycolyl transferase Major target antigen Protective in small animals In all environmental mycobacteria Doesn’t interfere with new diagnostic tests MVA85A BCG - MVA85A regimen
MVA85A can improve BCG induced protection in preclinical animal models MICE NHP Goonetilleke et al, JI 2003 Verreck et al, PLoS ONE 2009 GUINEA PIGS CATTLE Williams et al, I&I 2005 Vordermeier M et al, I&I 2009
Wk 1 Wk 2 Wk 8 Wk 24 Pre-MVA85A Pre-MVA85A Wk 1 Wk 2 Wk 8 Wk 24 MVA85A is highly immunogenic in UK trials McShane H et al, NM 2004 Beveridge N et al, EJI 2007 Sander C et al, AJRCCM 2009 Minassian A et al, BMJ Open 2011
MVA85A is immunogenic in South African trials Hawkridge A et al, JID 2008 Scriba T et al, EJI 2010 Scriba T et al, JID 2011
Co-administration of MVA85A with EPI vaccines reduces MVA85A immunogenicity in Gambian infants MVA85A + EPI MVA85A alone • 3 groups of infants: • EPI alone • EPI + MVA85A • MVA85A alone Ota et al, STM 2011
Infant Phase IIb efficacy trial • Objectives: • Safety • Immunogenicity • Efficacy (against disease & infection) • Immune correlates • Design: • BCG vaccinated infants in Worcester, South Africa • Randomised at 18-26 weeks to receive either: • MVA85A (1 x 108pfu) • placebo (Candin) • Sample size = 2784 (1392/arm) • Cumulative TB incidence of 3% • 90% power to detect 60% improvement over BCG alone • Status • Fully enrolled • 2 DSMB reviews • Due to unblind in Q4 2012
HIV safety data • No effect on HIV RNA load • No effect on CD4 count • AE profile as in HIV- subjects • No evidence of immune activation • No effect of MVA85A on CCR5 co-receptor expression • No change in unstimulated serum beta-chemokines • No higher levels of HIV gag DNA in Ag85A-specific cells than in CMV-specific cells • No evidence for bystander activation following MVA85A vaccination Minassian et al, BMJ Open 2011
A second MVA85A at 12 months enhances duration and magnitude of immunity in HIV-infected subjects * P < 0.05 Summed peptide pool responses Single peptide pool responses * * * * * * Dieye et al, unpublished data
Vaccine induced immune responses higher in subjects on ARVs Single peptide pool responses Summed peptide pool responses P<0.0138 ns P=0.0029 P=0.0027 P<0.0001 P=0.0024 P=0.0002 P=0.0003 Dieye et al, unpublished data
Phase IIb trial in HIV+ adults • Proof of concept study in HIV+ adults • protection against TB disease and M. tb infection • safety & immunogenicity • immune correlate samples stored • Two sites • South Africa: Cape Town (Robert Wilkinson) • Senegal: Dakar (Souleymane Mboup) • Design: • HIV-infected adults +/- ARV • 1400 subjects randomised to receive either: • 2 doses of MVA85A, 6-9 months apart or • 2 doses of placebo (candin) • Annual incidence assumed to be 2.5% • 80% power to detect 60% improvement • Follow-up for 2 years • Status: • Enrolment commenced August 2011
Progress • 14 vaccines evaluated in clinical trials • Two vaccines being evaluated in efficacy trials • No immunopathology issues identified in any clinical trials to date
Challenges • No immunological correlate • No validated animal models • Difficulty with end-points • Finite capacity to do efficacy testing
Funders and partners Oxford Emergent Tuberculosis Consortium European Commission Study participants