Download
1 / 1
10 likes | 224 Views
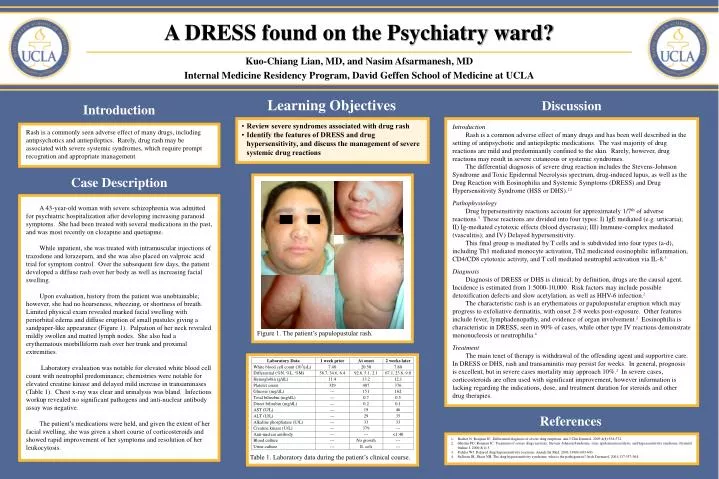
Figure 1. The patient’s papulopustular rash. Table 1. Laboratory data during the patient’s clinical course. A DRESS found on the Psychiatry ward? Kuo-Chiang Lian, MD, and Nasim Afsarmanesh, MD Internal Medicine Residency Program, David Geffen School of Medicine at UCLA. Learning Objectives.

E N D
Figure 1. The patient’s papulopustular rash. Table 1. Laboratory data during the patient’s clinical course. A DRESS found on the Psychiatry ward? Kuo-Chiang Lian, MD, and Nasim Afsarmanesh, MD Internal Medicine Residency Program, David Geffen School of Medicine at UCLA Learning Objectives Discussion Introduction • Review severe syndromes associated with drug rash • Identify the features of DRESS and drug hypersensitivity, and discuss the management of severe systemic drug reactions Introduction Rash is a common adverse effect of many drugs and has been well described in the setting of antipsychotic and antiepileptic medications. The vast majority of drug reactions are mild and predominantly confined to the skin. Rarely, however, drug reactions may result in severe cutaneous or systemic syndromes. The differential diagnosis of severe drug reaction includes the Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis spectrum, drug-induced lupus, as well as the Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) and Drug Hypersensitivity Syndrome (HSS or DHS).1,2 Pathophysiology Drug hypersensitivity reactions account for approximately 1/7th of adverse reactions.3 These reactions are divided into four types: I) IgE mediated (e.g. urticaria); II) Ig-mediated cytotoxic effects (blood dyscrasia); III) Immune-complex mediated (vasculitis); and IV) Delayed hypersensitivity. This final group is mediated by T cells and is subdivided into four types (a-d), including Th1 mediated monocyte activation, Th2 medicated eosinophilic inflammation, CD4/CD8 cytotoxic activity, and T cell mediated neutrophil activation via IL-8.3 Diagnosis Diagnosis of DRESS or DHS is clinical; by definition, drugs are the causal agent. Incidence is estimated from 1:5000-10,000. Risk factors may include possible detoxification defects and slow acetylation, as well as HHV-6 infection.2 The characteristic rash is an erythematous or papulopustular eruption which may progress to exfoliative dermatitis, with onset 2-8 weeks post-exposure. Other features include fever, lymphadenopathy, and evidence of organ involvement.2 Eosinophilia is characteristic in DRESS, seen in 90% of cases, while other type IV reactions demonstrate mononucleosis or neutrophilia.4 Treatment The main tenet of therapy is withdrawal of the offending agent and supportive care. In DRESS or DHS, rash and transaminitis may persist for weeks. In general, prognosis is excellent, but in severe cases mortality may approach 10%.2 In severe cases, corticosteroids are often used with significant improvement, however information is lacking regarding the indications, dose, and treatment duration for steroids and other drug therapies. Rash is a commonly seen adverse effect of many drugs, including antipsychotics and antiepileptics. Rarely, drug rash may be associated with severe systemic syndromes, which require prompt recognition and appropriate management. Case Description A 43-year-old woman with severe schizophrenia was admitted for psychiatric hospitalization after developing increasing paranoid symptoms. She had been treated with several medications in the past, and was most recently on clozapine and quetiapine. While inpatient, she was treated with intramuscular injections of trazodone and lorazepam, and she was also placed on valproic acid trial for symptom control. Over the subsequent few days, the patient developed a diffuse rash over her body as well as increasing facial swelling. Upon evaluation, history from the patient was unobtainable; however, she had no hoarseness, wheezing, or shortness of breath. Limited physical exam revealed marked facial swelling with periorbital edema and diffuse eruption of small pustules giving a sandpaper-like appearance (Figure 1). Palpation of her neck revealed mildly swollen and matted lymph nodes. She also had a erythematous morbilliform rash over her trunk and proximal extremities. Laboratory evaluation was notable for elevated white blood cell count with neutrophil predominance; chemistries were notable for elevated creatine kinase and delayed mild increase in transaminases (Table 1). Chest x-ray was clear and urinalysis was bland. Infectious workup revealed no significant pathogens and anti-nuclear antibody assay was negative. The patient’s medications were held, and given the extent of her facial swelling, she was given a short course of corticosteroids and showed rapid improvement of her symptoms and resolution of her leukocytosis. References • Bachot N, Roujeau JC. Differential diagnosis of severe drug eruptions. Am J Clin Dermtol. 2003;4(8):561-572. • Ghislan PD, Roujeau JC. Treatment of severe drug reactions: Stevens-Johnson Syndrome, toxic epidermal necrolysis, and hypersensitivity syndrome. Dermtol Online J. 2000;8(1):5. • Pichler WJ. Delayed drug hypersensitivity reactions. Annals Int Med. 2003;139(8):683-693. • Sullivan JR, Shear NH. The drug hypersensitivity syndrome: what is the pathogenesis? Arch Dermatol. 2001;137:357-364.