Download
1 / 44
610 likes | 1.19k Views
MANAGEMENT OF ABNORMAL PAP SMEAR. DR ALIFAH BT MOHD ZIZI O&G SPECIALIST SGH. BETHESDA SYSTEM 2001. It was designed to provide uniform diagnostic language to facilitate communication between cytologists and clinician 3 general categories Within Normal Limits

E N D
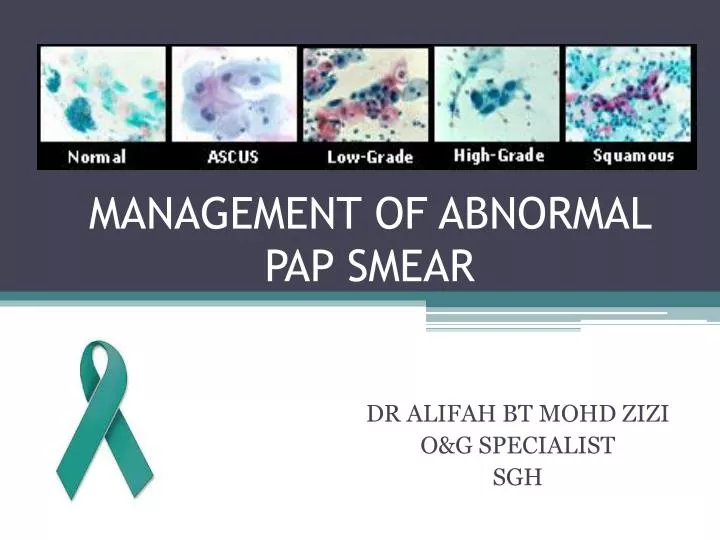
MANAGEMENT OF ABNORMAL PAP SMEAR DR ALIFAH BT MOHDZIZI O&G SPECIALIST SGH
BETHESDA SYSTEM 2001 • It was designed to provide uniform diagnostic language to facilitate communication between cytologists and clinician • 3 general categories • Within Normal Limits • Benign Cellular Changes • Epithelial Cell Abnormality
BETHESDA SYSTEM 2001 • Adequacyof the sample is paramount • 8000 – 12,000 squamous cells for conventional PS/10 HPF • 5000 cells/10 HFP for liquid-based sample • Presence of endocervical cells (at least 10) is recommended (not required for women < 40 y.o)
WHAT IS ABNORMAL PAP SMEAR? • Abnormal due to inadequacy • Abnormal due to inflammation • Abnormal due to infection • Abnormal due to dysplastic changes
SATISFACTORY SPECIMEN.. • Appropriate labeling and identifying information • Relevant clinical information • Adequate numbers of well preserved and well visualized squamousepithelial cells. • An adequate endocervical / transformation zone component (from a patient with a cervix). • Quality of the Pap smear will still be noted when: 1. More than 10 well preserved endocervical or metaplatic cells are seen 2. No blood or inflammation obscuring the Pap smear
INADEQUATE/UNSATISFACTORY SMEAR • A smear that is unreliablefor the detection of cervical epithelial cell abnormalities
INADEQUATE/ UNSATISFACTORY SMEAR 1. Sampling Scanty cells Blood, mucous, pus 2.Preparation Too thick due to poor spreading Air drying artifact Broken slide 3.Mainlyendocervical cell
HOW TO DEAL WITH INADEQUATE/UNSATISFACTORY SMEAR ?? • Correct timing of smear • Correct timing of smear • Do not use cream or gel • Cleaning of excessive mucus • Choice of sampling devices • Correct spreading • Rapid fixation (< 10 second) • Correct timing of smear • Do use cream or gel
PAP SMEAR UNSATISFACTORY • TX ANY INFECTION • GIVE A COURSE OF ESTROGEN IF POST MENOPAUSE WITH ATROPHY REPEAT 6/12 NEGATIVE FOR INTRAEPITHELIAL LESSION 2ND SMEAR UNSATISFACTORY REPEAT 6/12 3RD SMEAR UNSATISFACTORY ROUTINE SCREENING COLPOSCOPY
Inflammation on Pap smear results, does not indicate any particular pathology • Therefore, does not necessitate routine treatment.
POSSIBLE CAUSES…… • Infection • Chronic cervicitis • Atrophic cervicitis • Chemical or mechanical irritation to cervix- tampoon, douching
PAP SMEAR NEGATIVE FOR MALIGNANT CELL INFLAMMATORY TX ANY INFECTION OR ATROPHY REPEAT 6/12 NORMAL 2ND SMEAR INFLAMMATORY REPEAT 6/12 ROUTINE SCREENING 3RD SMEAR INFLAMMATORY COLPOSCOPY
COMMON INFECTIONS…. • Tricomonasvaginalis • Fungal iecandidiasis • Bacterial Vaginosis • Actinomyces • Herpes Simplex
PAP SMEAR NEGATIVE FOR MALIGNANT CELL SPECIFIC MICROORGANISM TREAT ANY INFECTION REPEAT PAP SMEAR 6/12 NORMAL ROUTINE SCREENING
DYSPLASTIC CHANGES SQUAMOUS CELL ABNORMALITY GLANDULAR ABNORMALITY • AGS • AIS • INVASIVE ADENOCARCINOMA • ASCUS • ASC-H • LGSIL • HGSIL • INVASIVE SQUAMOUS CELL CARCINOMA
Spectrum of Changes in Cervical Squamous Epithelium Caused by HPV Infection HPV Infection/ CIN* 1 CIN 2 / CIN 3 / Cervical Cancer Normal Cervix *CIN = cervical intraepithelial neoplasia Adapted from Goodman A, Wilbur DC. N Engl J Med. 2003;349:1555–1564.
ABNORMAL PAP SMEAR DUE TO DYSPLASTIC CHANGES – SQUAMOUS CELL ABNORMALITIES 1. Atypical Squamous Cells (ASC) • Atypical Squamous Cells-Undetermined Significance (ASC-US) • Atypical Squamous Cells, Cannot Exclude High Grade Lesion (ASC-H) 2. Low-grade Squamous Intraepithelial Lesion (LSIL) (Mild Dyskaryosis / HPV/CIN 1) 3. High-grade Squamous Intraepithelial Lesion (HSIL) (Mod or Severe Dyskaryosis / CIN 2,3) 4. Invasive Squamous Cell Carcinoma
1.ATYPICALSQUAMOUS CELL (ACS) 1. Undetermined Significance (ASC-US) • Cytologic changes suggestive of a low grade squamous lesion but lack criteria for definitive interpretation. 2. Cannot Exclude High Grade Lesion (ASC-H) • Cytologic changes suggestive of a high grade squamous lesion but lack criteria for definitive interpretation.
PAP SMEAR ATYPICAL SQUAMOUS CELL (ASC) ASCUS HPV DNA TESTING POSITIVE NEGATIVE REPEAT 6/12 COLPOSCOPY NEGATIVE FOR INTRAEPITHELIAL LESSION RESUME NORMAL SCREENING
PAP SMEAR ASC-H COLPOSCOPY
2. LOW GRADE INTRAEPITHELIAL LESSION (LGSIL) / CIN 1 • CINI being the morphologic manifestation of a self-limited sexually transmitted HPVinfection • 60% of CIN I regress spontaneously • 30% of CIN I persists. • 10% of CIN I lesions progress to CIN III, • 1% may ultimately progress to invasive cancer.
= No yes Assessment of client • Presence of at least 1 criteria: • -Age > 30 yrs • Poor compliance • Immunocompromised • Sx • Hx of pre-invasive lesion • +ve for high risk HPV • (16,18,31,33,45,52,58) Repeat smear in 6/12 60% NILM LSIL Immediate colposcopy Resume routine screening schedule Colposcopy
MANAGEMENT APPROACH • A lesion that persist after 1-2 years or any progression during follow up suggest need of treatment • If HPV testing is available, +veHPV: indication for treatment - Treatment- local ablative/ excission -Follow up after treatment for CIN1 -repeat smear in 6/12 -repeat smear and colposcopy in 12/12 -If normal, yearly pap smear x 2 years then back to normal routine
3.HIGH GRADE INTRAEPITHELIAL LESSION (HGSIL)/ CIN 2-3 • CIN 2-3 is a cervical cancer precursor 1.CIN 2 • 40%of CIN II regress • 30% of CIN II persist • 20% of CIN II progress to CIN III • 5% of CIN II progress to CINIII 2. CIN 3 • 33% of CIN III regress • 18% of CIN III progress to invasive disease over a 10 years • 36% of CIN III progress to invasive disease over a 20 years
PAP SMEAR HGSIL COLPOSCOPY AND BIOPSY • Subsequent management depends on: • Whether lesion identified • Whether colposcopy satisfactory • Annual smear following treatment
MANAGEMENT APPROACH EXCISION METHOD • LLETZ • Cold knife cone biopsy • Hysterectomy
ABLATIVE METHODS • Cryocautery • Electrodiathermy • Cold coagulation
4. INVASIVE SQUAMOUS CELL CANCER PAP SMEAR INVASIVE SQUAMOUS CANCER COLPOSCOPY AND BIOPSY • Subsequent management depends on: • Stage of the disease
ABNORMAL PAP SMEAR DUE TO DYSPLASTIC CHANGES- GLANDULAR CELL ABNORMALITIES 1.AtypicalGlandular Cells (AGS) (undetermined or favourneoplastic) 2.Adenocarcinomain Situ (AIS) 3. Invasive Adenocarcinoma
GLANDULAR ABNORMALITIES • The most common significant lesions associated with AGC (Atypical Glandular Cells) are actually squamous • Management should include colposcopyand endocervical sampling
ATYPICAL ENDOMETRIAL CELLS • Always perform endometrial sampling • If endometrial sampling is negative :colposcopywith endocervical sampling
ATROPHY SMEAR PAP SMEAR ATROPHY LOCAL ESTROGEN CREAM 1G ON FOR 2 WEEKS THEN TWICE WEEKLY FOR 6 WEEKS REPEAT IN 6 MONTHS
REACTIVE CELLULAR CHANGES PAP SMEAR REACTIVE CELLULAR CHANGES DUE TO RADIATION, REPAIR OR IUCD REPEAT IN 1 YEAR
ABNORMAL PAP SMEAR IN PREGNANCY • Reported abnormal smear during pregnancy 1%- 8% • Follow-up should be similar to non pregnant state-every trimester • Regardless of gestation, suspicious lesion should be biopsied. • Cervical biopsy does not increase the risk of miscarriage • If evidence of invasive cancer- require excission