Download
1 / 36
370 likes | 622 Views
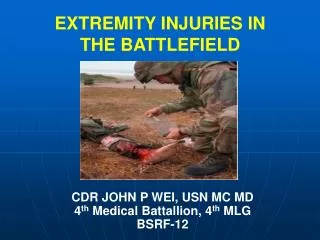
TRAUMA LESSONS FROM THE BATTLEFIELDS OF AFGHANISTAN AND IRAQ. CDR JOHN P WEI, USN MC MD 4th Medical Battalion, 4th MLG BSRF-12. BATTLEFIELD TRAUMA. Changes in epidemiology of combat injuries in current military conflicts Lessons learned from care of trauma victims in Afghanistan and Iraq

E N D
TRAUMA LESSONS FROM THE BATTLEFIELDS OF AFGHANISTAN AND IRAQ CDR JOHN P WEI, USN MC MD 4th Medical Battalion, 4th MLG BSRF-12
BATTLEFIELD TRAUMA • Changes in epidemiology of combat injuries in current military conflicts • Lessons learned from care of trauma victims in Afghanistan and Iraq • Transfer relevant lessons to civilian medical practice
25% 10% 9% 5% 12% 7% 31% 1 % Causes of Death in Ground Combat KIA : CNS injury KIA : Airway obstruction KIA : Blast / mutilating trauma KIA : Tension PTX KIA : Torso trauma, not correctable KIA : Torso trauma, correctable KIA : Extremity exsanguination DOW : Infection, shock complications (KIA = Killed in Action ; DOW = Died of Wounds)
Causes of Death in Ground Combat KIA: CNS injury KIA: Airway obstruction 25% 10% KIA: Blast / mutilating trauma 9% KIA: Tension PTX 5% KIA: Torso trauma, not correctable 12% 7% 31% KIA: Torso trauma, correctable 1% KIA: Extremity exsanguination DOW: Infection, shock complications 15% of Deaths Preventable in Field
Routine Use of Individual Body Armor (IBA) by the U.S. Military Current issued U.S. Army IBA Neck, shoulder, and groin flaps Use of IBA accounts for the decrease in torso wounds and the increase in the percentage of extremity wounds Use of polycarbonate protective eyewear
CARE FOR INJURIES IN BODY ARMOR With no skin penetration, internal injuries can occur from a bullet striking armor If hit on chest : lung contusion, rib fracture possible keep patient under observation, repeat chest x-ray at 4 to 6 hours If lower chest or abdomen hit : may be spleen or liver contusion or laceration Kevlar armor impossible to cut with standard trauma scissors
LIFE SAVING FIELD INTERVENTIONS Stop external hemorrhage Extremity tourniquets safe and effective Needle decompression of tension pneumothorax in dyspneic patient Provide airway in unconscious patient Nasopharyngeal or oral airway efficacious
CPR ON BATTLEFIELD Utility of CPR in field: drowning hypothermia electrical shock No benefit with mass casualties involving limited resources
PRIORITIES OF TRAUMA Life > priority over sight> limb Exsanguinating hemorrhage > priority over airway Torso injury > priority over limb Pulseless limb > priority over limb with pulse Open fracture > priority over closed fracture
MEDICAL LESSONS FROM BATTLEFIELD Clinical experience in dealing with blast and explosive injuries New strategies in treating hemorrhage Mortality rates lower for the current conflicts Survivors of massive multiple trauma with major deficits
PRIOR U.S. MILITARY MEDICAL EXPERIENCE Mortality Rates After Wounding : Revolutionary War : 42 % World War II : 30 % Korean War : ~25 % Vietnam War : ~25 % Persian Gulf War : ~25 % Iraq and Afghanistan: < 10 %
CURRENT U.S. MILITARY MEDICAL EXPERIENCE Medical advances from current conflicts: Treatment of primary and secondary blast injury Use of damage control surgery Blood and activated clotting factors Tourniquets Hemostatic agents and dressings
CASUALTIES FROM IED (Improvised Explosive Devices) Predominance of current injuries in Afghanistan Severe, multisystem Multiple limb amputations Secondary injury from being thrown Eardrum rupture Occult injuries: blast lung, bowel rupture, traumatic head injury
CATEGORIES OF BLAST INJURIES Primary : blast pressure on organs and tissue Secondary : injuries from projectiles Tertiary : blunt trauma from patient thrown against hard object Miscellaneous : burns, crush, toxic inhalations
POTENTIAL INJURIES IN BLAST VICTIM Respiratory Pulmonary hemorrhage Alveolar-venous fistula air embolism production Airway epithelial damage Circulatory Cardiac contusion Air embolism myocardial ischemia
POTENTIAL INJURIES IN BLAST VICTIM Digestive tract Gastrointestinal hemorrhage or perforation Retroperitoneal hemorrhage Ruptured spleen or liver Eye and Orbit Retinal air embolism Orbital fracture
POTENTIAL INJURIES IN BLAST VICTIM Auditory system Tympanic membrane rupture Ossicular fractures Cochlear damage
POTENTIAL INJURIES IN BLAST VICTIM Perform ear exam If TM rupture obtain chest x-ray, hold for 8 hour observation If TM not ruptured, no other symptoms conditionally exclude other serious primary blast injury Pulse oximetry : O2 saturation signals early blast lung before symptoms develop
DAMAGE CONTROL SURGERY Technique widely used in theater Central tenet: avoid “ The Deadly Triad” Hypothermia Coagulopathy Metabolic acidosis Mortality and morbidity increases with additional risk factors
DAMAGE CONTROL SURGERY Stop the bleeding Close gastrointestinal leaks Remove major contaminants Leave wound open to avoid abdominal compartment syndrome Transfer to Intensive Care Unit (ICU) for further stabilization and resuscitation
DAMAGE CONTROL SURGERY Resuscitate in ICU Normalize blood pressure Normalize body temperature Normalize coagulation factors Return to Operating Room when stable for definitive surgery
HEMOSTASIS International Normalized Ratio (INR) > 1.5 on arrival is predictive of need for massive transfusion Thawed fresh frozen plasma (FFP) is best resuscitation fluid in MT Optimum ratio of plasma : crystalloid is 1:1 to avoid clotting factor dilution > 50 %
HEMOSTASIS Limit crystalloid use in the field : Overuse can lead to inflammatory, acidotic, coagulopathy effects Hextend (hetastarch) suitable for field use give 500 cc, repeat once if hemorrhage Use fresh whole blood; not available, use one unit of FFP for each unit of banked packed cells Early use of cryoprecipitate Recombinant Factor VIIa (rFVlla) TXA (transamenic acid) for coagulopathy
HEMOSTASIS Tourniquets : Use for any significant extremity hemorrhage No adverse events seen Use early Issued to every soldier The Combat Application Tourniquet (CAT) can be applied by an injured soldier to himself using only one hand
HEMOSTASIS Hemostatic dressings : Avoid coagulopathy : control bleeding early Used for non-extremity hemorrhage, but also in severely mangled limbs Apply with pressure < 5 minutes, patient stabilized and evacuated
HEMOSTASIS HemCon (chitosan) Originally as bandage Now in roll that can be stuffed into wound QuikClot (initially available as a powder ; subsequently marketed in a adherent package) Very exothermic (up to 147 o F) Difficult to debride from wound due to adherence New Advanced Clotting Sponge (ACS) Gauze sack : is easily removed from wound
MEDICATIONS IN FIELD • Medical providers carry oral antibiotics (gatifloxacin 400 mg per day currently used) and pain meds (Celebrex 200 mg per day and / or acetominophen) • Cefotetan 2 grams IV or IM for severely injured
SUMMARY Body armor has changed injury patterns Tourniquets are lifesaving for exsanguinating extremity wounds Early antibiotics in the field are indicated Fresh whole blood and plasma are best resuscitation fluids Damage control surgery is effective for the massively injured Blast victims have multiple, occult, and delayed injuries