Download
1 / 22
250 likes | 423 Views
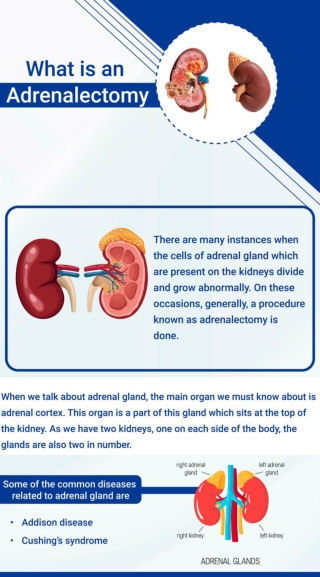
Endocrine Adrenal gland. Adrenal glands: The adrenal glands are paired endocrine organs consisting of both cortex and medulla, which differ in their development, structure, and function. The adrenal cortex synthesizes three different types of steroids:

E N D
Adrenal glands: The adrenal glands are paired endocrine organs consisting of both cortex and medulla, which differ in their development, structure, and function. The adrenal cortex synthesizes three different types of steroids: (1) glucocorticoids (principally cortisol) (2) mineralocorticoids, the most important being aldosterone (3) sex steroids (estrogens and androgens) The adrenal medulla is composed of chromaffin cells, which synthesize and secrete catecholamines, mainly epinephrine.
Adrenal glands: Hypercortisolism (Cushing Syndrome) Exogenous Endogenous divided into those that are • ACTH dependent • ACTH independent Adrenal insufficiency(hypoadrenalism) primary (Addison disease) secondary
Hypercortisolism (Cushing Syndrome) Pathogenesis: • This disorder is caused by any condition that produces elevated glucocorticoid levels. Cushing syndrome can be broadly divided into exogenous and endogenous causes. • The vast majority of cases of Cushing syndrome are the result of the administration of exogenous glucocorticoids (“iatrogenic” Cushing syndrome). • The endogenous causes can, in turn, be divided into those that are ACTH dependent and those that are ACTH independent
Depending on the cause of the hypercortisolism the adrenals have : In patients in whom the syndrome results from exogenous glucocorticoids, suppression of endogenous ACTH results in bilateral cortical atrophy, due to a lack of stimulation of the adrenal by ACTH. In contrast, in cases of endogenous hypercortisolism, the adrenals either are hyperplastic or contain a cortical neoplasm.
The main lesions of Cushing syndrome that are found in the pituitary and adrenal glands: (Pituitary gland changes in cushing syndrome) • Crock hyaline changes: This is the most common change seen in pituitary gland in all forms of cushing syndrome. In this condition, the normal granular, basophilic cytoplasm of the ACTH producing cells in the pituitary is replaced by homogenous, lightly basophilicmaterial (cytokeratin filaments deposition). • Pituitary Adenomas or foci of ACTH cell hyperplasia.
A patient with Cushing syndrome demonstrating central obesity, “moon facies,” and abdominal striae
Causes of chronic primary hypoadrenalism (Addison disease) • Autoimmune diseases. • Tuberculosis. • AIDS • Metastatic diseases • Fungal infection • Sarcoidosis • Systemic amyloidosis.
AddisonDisease. • Is uncommon disorder resulting from progressive destruction of the adrenal cortex. • Clinical features of Addison disease do not appear until at least 90% of adrenal cortex has been destructed.
Morphology of hypoadrenalism Gross. In Addison disease, adrenal glands are shrunken; while in secondary hypoadrenalism (due to diseases of pituitary & hypothalamus) adrenal glands are reduced to small, flattened, yellow structure. Mic. In Addison disease, the cortex of adrenal glands contains only scattered residual cortical cells within the network of connective tissue, with lymphoid infiltration of the cortex.
Clinical features of Addison disease: • Insidious onset of weakness & easy fatigability. • ↑K,↓Na,↓BP, due to mineralocorticoid insufficiency. • Hyperpigmentation in primary hypoadrenalism (due to increase level of POMC precursor to ACTH and melanocytes stimulating hormone). • Nausea, vomiting & diarrhea. • Hypoglycemia & glycosuria. • Acute stresses (e.g., trauma or infection) • can precipitate acute adrenal crisis, with rapid progression to deathunless corticosteroid therapy is promptly initiated.
Patients with Addison disease have diffuse hyperpigmentationas well as hyperpigmentation on extensor surfaces (here the elbows) as in the top left panel. In the top right panel, hyperpigmentation of the palmar creases is visible in a patient with Addison disease. In the bottom left panel hyperpigmentedmacules of the gums are visible in this patient with Addison disease. Some patients with Addison disease have vitiligo and hyperpigmentation as seen in the bottom right panel.
Pathology of adrenal medulla. The most important pathological process in adrenal medulla is Pheochromacytoma Pheochromacytoma: Are neoplasm composed of chromaffin cells, which like the non neoplastic chromaffin cells synthesize & release catecholamines (epinephrine, norepinephrine). Pheochromacytoma can describe by a rule of 10s • 10% of pheochromacytoma are familial. • 10% are extra- adrenal in their sites (Paraganglioma). • 10% of cases are bilateral. • 10% are biologically malignant.
Gross. • Range from small, circumscribed to large hemorrhagic mass. Mic. • Composed of polygonal to spindle cells with their supporting cells, which divide the tumor into small nests (zellaballen) pattern by a rich vascular network. • Cytoplasm of neoplastic cells is granular (due to their contents of catecholamines granules). • Even in benign cases, there is vascular & capsular invasion, so the diagnosis of malignant pheochromacytoma depends onpresence of metastases (to lymph nodes, lung, liver, & bones).
Clinical features. • The most characteristic clinical feature of pheochromacytoma is isolated, paroxysmal, episodes of hypertension in 50% of cases, with associated symptoms like (tachycardia, palpitation, headache, tremor, sudden abdominal symptoms). • All these symptoms are due to overproduction of catecholamines by the neoplastic cells. • Laboratory data (increase urinary excretion of free catecholamines & their metabolites like Vanilyl Mndelic Aid (VMA).
Pheochromocytoma. The tumor is enclosed within an attenuated cortex and demonstrates areas of hemorrhage. The comma-shaped residual adrenal is seen below
Pheochromocytoma demonstrating characteristic nests of cells with abundant cytoplasm. Granules containing catecholamine are not visible in this preparation. It is not uncommon to find bizarre cells even in pheochromocytomas that are biologically benign