Download
1 / 55
690 likes | 1.33k Views
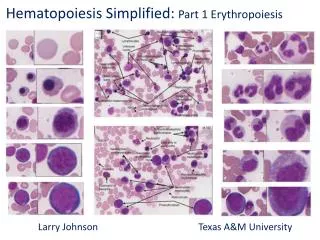
Normal and abnormal Barrett W. Dick, M.D. Director, Hematology Laboratories Memorial Medical Center Springfield. IL Clinical Professor, Pathology and Medicine Southern Illinois School of Medicine. ERYTHROPOIESIS. RBC development. Increasing cytoplasmic hemoglobin.

E N D
Normal and abnormal Barrett W. Dick, M.D. Director, Hematology Laboratories Memorial Medical Center Springfield. IL Clinical Professor, Pathology and Medicine Southern Illinois School of Medicine ERYTHROPOIESIS
RBC development Increasing cytoplasmic hemoglobin Decreasing cytoplasmic RNA
POLYCHROMATOPHILIA VS. NORMAL IMMATURE MATURE Immature red cells are bigger, bluer and have less central pallor than mature rbc. NOTE: On the left is a diagrammatic representation of a young red cell, usually described as “polychromatophilic”. Note that it is larger and bluer than a mature red cell on the right. This is due to its RNA content.
Reticulocytes vs. Polychromasia • Reticulocytes require special techniques for measurement • The two terms are not equivalent but frequently, but incorrectly, used as equivalent • Estimating polychromasia from a stained blood smear is not a substitute for performing a reticulocyte count. The correlation is poor.
Increased Polychromasia PolychromatophilicRbc
Blood Smear Examination Too thick Too thin Area behind “feather edge”- Just right.
Smear Examination Thin Area Feather Edge
Low Power Examination Of Blood Smear • Performed at 10X magnification • Evaluate quality of smear- appropriate thin area • Check for increased rouleaux formation • Scan for white cell distribution- even • With practice can estimate the white count and differential: at very least make sure they correlate with machine count and/or manual diff
Thin Area of Smear 10X mag
Ideal Area of Blood Smear Red cells close, evenly spaced without significant overlapping 50X Oil
Increased Rouleaux Formation Some degree of rouleaux formation is normal; this is increased
High Power Examination • Scan performed at no lower than 40X coverslipped smear or 50X oil • Estimate the differential and look for qualitative Wbc abnormalities • Rbc morphology • Platelet estimate • Perform a differential at 100X if specimen has been flagged as being abnormal- 200 cells.
Rbc variation • Anisocytosis- Variation in size • Poikilocytosis- Variation in shape • Slight variation of size and shape is normal. When abnormalities are reported, what it should mean is that more than normal variation is present.
Normal Size Distribution RBC 50 100 200 NOTE: This illustrates a normal red cell distribution with the horizontal scale representing cubic micra. The RDW is by convention a mathematical expression of the width of the curve near the base.
Red Cell Size • Red cell size can only be measured accurately using electronic instrumentation to measure the volume (MCV). • On blood smear examination, the size estimate is based on diameter, which is not very accurate and does not correlate well with the MCV • Small lymphocyte nuclei are a rough guide to normal Rbc diameter
Microcytic Rbc 7.5 mu Avr.diameter of normal Rbc= 7.5 mu
Microcytic Hypochromic Rbc • Hypochromia is the most frequently overcalled abnormality on blood smears, usually due to technical factors • When real, usually due to advanced iron deficiency • Men: Hgb<10g/dl • Women: Hgb<8g/dl • Rarely in our population- thalassemia major
Macrocytic Rbc This smear also illustrates increased variation in size (anisocytosis) and increased variation in shape (poikilocytosis).
Elliptocytes (ovalocytes) Elliptocytes are a common non-specific abnormality. Hereditary elliptocytosis is also relatively common and is usually not hemolytic. The hereditary form is more common in peoples of African origin
Burr Cells, Acanthocytes, Crenated Cells • Terms that are frequently, but incorrectly, used interchangeably. When strictly defined the terms can have specific clinical correlations. Burr Cell Acanthocyte Crenated Rbc
Burr Cells Burr cells have rounded, blunt projections at the edges and have central pallor
Burr Cells • Uremia • Liver disease • Metabolic imbalance
Acanthocytes Acanthocytes look like spherocytes with irregularly spaced, thin, spiny projections
Differential Dx for Acanthocytes • Liver Disease • Post-Splenectomy • aBeta lipoproteinemia
Crenated Red Cells Crenated red cells have the appearance of sea urchin eggs: short, evenly-spaced, broad-based spikes projecting in three dimensions. They are seen in some severely ill patients with marked electrolyte abnormalities. In a reference laboratory setting, they are a frequent manifestation of a poorly preserved specimen..
Post-Splenectomy • Howell-Jolly Bodies • Acanthocytes • Target Cells • Lymphocytosis
Post-Splenectomy Howell-Jolly Body
Target Cells • Liver disease and/or hyperbilirubinemia • Post-splenectomy • Hemoglobinopathies • Hemoglobin C syndromes: • AC, SC, C-thal • NOT thalassemia minor, <1% of cases
Spherocytes The cells are small in diameter but not in volume. Because of their spherical shape they do not flatten on the slide.
Differential Dx- Spherocytes • Hereditary Spherocytosis • Autoimmune hemolysis • Alloimmune hemolysis- • Newborns with ABO incompatibility • Delayed transfusion reactions • Thermal injury- burn patients • Occasionally- non-specific with transfused red cells
Tear Drop Cells Common in disorders associated with marrow infiltration and splenomegaly
Coarse Basophilic Stippling Coarse stippling is usually associated with some form of dyserythropoeisis.
Schistocytes- Rbc fragments, so-called “Microangiopathic Hemolytic Anemias” • TTP /HUS • Vasculitis • Partially thrombosed vessels including heart chambers • Sever cardiac valve abnormalities or malfunctioning prosthesis • DIC- rarely; most often associated with chronic DIC
Pocked (Pitted”) Red Cells These cells look like spherocytes with bites in the edges, aka, “bite” cells. This is due to removal of denatured hemoglobin by the pitting function of the spleen
Heinz Body Hemolytic Anemias • Heinz Bodies are denatured hemoglobin usually due an oxidant. They are removed by the spleen causing deformed rbc- “pitted” rbc, aka “pocked” or “bite” cells • Hereditary • G6PD deficiency: hemolysis is usually drug induced or can be induced non-specifically by stress, such as infection • Unstable hemoglobins • Acquired: oxidant drug-induced without a hgb or enyzmatic abnormality
Common Hemoglobinopathies with Peripheral Blood Abnormalities • Thalassemia minor- microcytosis with mild or no anemia; worldwide in distribution • Hemoglobin AC- Target cells, sometimes spherocytes (few); from West Africa • Hemoglobin AE or EE- Microcytosis and target cells with minimal or no anemia: from SE Asia • Hemoglobin SS- Sickle cells with variable anemia • Hemoglobin SC- Target cells, spherocytes, sometimes sickle cells depending on the severity; may be asymptomatic
Thalassemia minor Mild or no anemia with microcytosis. The prevalence of target cells in this disorder is markedly overstated in texts and in the literature
S-C Disease SC crystals have a characteristic appearance with blunted, rhomboidal ends
Screening for Hemoglobinopathies • Thal minor CANNOT be diagnosed by Hgb electrophoresis in the overwhelming majority of patients; it is a diagnosis of exclusion: R/O iron deficiency • Hemoglobin electrophoresis is the procedure of choice for testing for other hemoglobin abnormalities; quick tests are not recommended