Download
1 / 19
200 likes | 386 Views
Update on HIV and infant feeding. Peggy Henderson and Constanza Vallenas Department of Child and Adolescent Health and Development, WHO Rome, 25 February 2007. UN Recommendations. HIV- women or HIV status unknown

E N D
Update on HIV and infant feeding Peggy Henderson and Constanza Vallenas Department of Child and Adolescent Health and Development, WHO Rome, 25 February 2007
UN Recommendations HIV- women or HIV status unknown • Exclusive breastfeeding for 6 months and continued breastfeeding for 2 years or beyond HIV+ women • Most appropriate infant feeding option for HIV-exposed infant depends on individual circumstances, including consideration of health services, counselling and support
Selecting an option:AFASS To be a better option for the individual than exclusive breastfeeding, replacement feeding has to be AFASS: • Acceptable • Feasible • Affordable • Sustainable AND • Safe For the mother and baby
Balancing risksfor HIV-positive women HIV transmission IF BREASTFEEDING Mortality Infectious diseasesMalnutrition IF NOT BREASTFEEDING
Balancing risks - 1 HIV transmission Risk of HIV transmission with full package of MTCT prevention Interventions(HAART, replacement feeding, caesarean section)< 2% Risk of HIV transmission through breastfeeding: • Exclusive breastfeeding (6 weeks – 6 months) ~ 4% • Breastfeeding as usual (varying duration) 5 to 20%
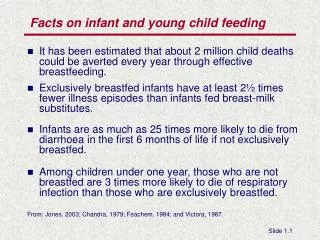
Balancing risks – 2Relative risk of infectious disease mortality among non-breastfed infants 5.8 Relative risk 4.1 2.6 1.8 1.4 Age (months) WHO Collaborative Study Team, Lancet, 2000
Balancing risks – 3Mixed feeding carries higher risk of HIV transmissionthan exclusive breastfeeding Hazard ratio Coovadia et al., Lancet, in press
Balancing Risks - 4No Difference in 18-Month mortality/HIV infection between Formula and Breastfed Infants FF: 33 infected, 62 deaths BF: 53 infected, 48 deaths p=0.60 p=0.86 p=0.08 % HIV-Infected or Dead Thior et al., JAMA, 2006
Supporting a mother to choose and implementan option:Before delivery and in the first months • Counselling based on broad definition of AFASS for her and her baby • 2 main options (replacement feeding and exclusive breastfeeding for 6 months), with other local options discussed only if mother interested • Support for choice
High EXCLUSIVE breastfeeding rates achievable with good quality counselling and support Median duration of EBF = 159 days Coovadia et al., Lancet, in press
Emerging evidence • Early BF cessation associated with increased morbidity and mortality in HIV-exposed infants • Providing free infant formula from birth does not necessarily lead to better HIV-free survival compared to EBF
Infant infections by feeding mode Vertical Transmission Study, in Press
Emerging evidence • HIV-positive infants benefit from continued BF • Availability of health system support important in assessing AFASS • Severity of disease in mother important, but AFASS criteria still more critical
Emerging evidence • Improved adherence, longer duration of exclusive breastfeeding achieved in HIV-infected and HIV-uninfected mothers given consistent messages and frequent, high quality counselling • Not enough evidence re ARVs and breastfeeding to draw firm conclusions, but HIV-infected mothers who need ARVs should have them
Supporting a mother at key decision points in first months • If mother breastfeeding: • Early testing (PCR): • Baby HIV-negative: replacement feeding if AFASS • Baby HIV-positive: continue breastfeeding • Improvement in financial/social/support situation: re-assess AFASS to consider replacement feeding • Mother on ARVs: Risk of transmission low, but replacement feeding if AFASS • Continued support for choice for all mothers
Supporting a mother when practiceschange at 6 months • If still breastfeeding: • if other milks, animal source-foods available – cease all breastfeeding and give other foods • no such foods available – risk of mixed feeding for a few months probably less than risk of severe malnutrition • If breastfeeding already stopped: • Continue with milk of some kind and complementary foods • Continued support for choice
Implications for scaling-up in countries • Good quality infant feeding counselling and support for mothers (training, motivation, supervision) • Protection, promotion and support for infant feeding for all women to help HIV-positive women who breastfeed • Where breast-milk substitutes provided, safe and appropriate use and prevention of spillover • Link infant feeding with effective reproductive and child health services
Updating guidance • Consensus Statement from 2006 Technical Consultation (new evidence and experience, updated recommendations • Full consultation report (1st quarter 2007) • Update of Review of transmission (1st quarter 2007) • Technical update (2nd quarter 2007) • Minimal revision of existing tools (as reprinted) • Complete revisions when more evidence on ARVs and breastfeeding available (~2008-9)