Download
1 / 26
260 likes | 425 Views
Hope in the TB Pipeline II: Vaccines. Peg Willingham Aeras Global TB Vaccine Foundation. J2J Lung Health Media Training 41st Union World Conference on Lung Health Berlin, Germany 12 November 2010. Existing TB Vaccine Ineffective. BCG introduced in 1921.

E N D
Hope in the TB Pipeline II: Vaccines Peg Willingham Aeras Global TB Vaccine Foundation J2J Lung Health Media Training 41st Union World Conference on Lung Health Berlin, Germany 12 November 2010
Existing TB Vaccine Ineffective BCG introduced in 1921 • BCG unreliable against pulmonary TB, which accounts for most TB disease worldwide • BCG is not know to protect against latent TB • BCG is not recommended for use in infants infected with HIV - increased risk for severe BCG-related complications • Despite wide use, BCG has had no apparent impact on the growing global TB epidemic • BCG does reduce risk of severe pediatric TB disease, so it should continue to be used until a better TB vaccine is available
Tuberculosis: TB Vaccine Too Dangerous for Babies With AIDS Virus, Study Says July 2, 2009 – The vaccine against tuberculosis that is routinely given to 75 percent of the world’s infants is too risky to give to those born infected with the AIDS virus, says a new study published by the World Health Organization. It recommended that vaccination be delayed until babies can be tested.
Children with HIV infection regardless of symptoms should not be BCG vaccinated All high risk infants need HIV screening Maternal antibody masks antibody tests Detection of virus required Very difficult to implement in many places WHO 2007 Recommendations on BCG • Disseminated BCG in HIV infected infants recently (2009) estimated to be 992 per 100,000 (Hesseling, et al)
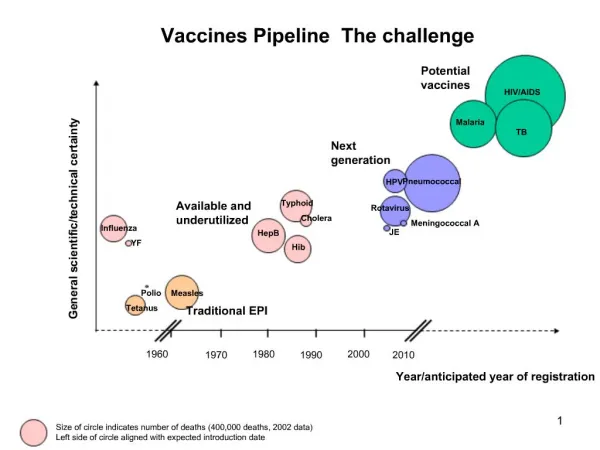
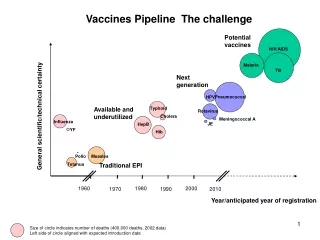
Predicted Impact of 50% Effective New TB vaccine Young and Dye Cell 2006
Goals for Better TB Vaccines Eliminate TB as a public health threat, in line with global targets (<1 case/million), in conjunction with new drugs and diagnostics Safe and effective in preventing TB in children, adolescents and adults, including people with HIV (for whom BCG is unsafe) Protect against all forms of TB – including MDR and XDR
TuBerculosis Vaccine Initiative (TBVI) • European efforts to develop more effective, safe vaccines against tuberculosis, that will be globally accessible and affordable. • R&D support and Advocacy • Focus: • Discovery • Preclinical • Phase I/IIa - early clinical stages
Aeras Global TB Vaccine Foundation Mission To develop new, more effective TB vaccines and ensure their availability to all who need them Method Non-profit PDP; collaborate with academic, biotech, pharma and NGO partners to develop and test new TB vaccines Pursue a Prime-Boost strategy by developing a modern replacement for BCG plus booster vaccines Develop vaccines in our own lab and manufacturing plant
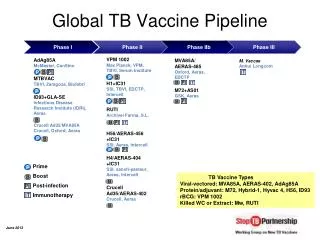
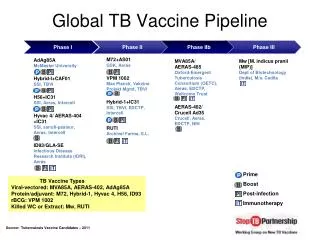
TB Vaccine Pipeline As of November 2009 Preclinical Phase I Phase II Phase IIb Phase III AERAS-422Aeras Mtb [∆lysA ∆panCD ∆secA2]Albert Einstein College of Medicine MTBVAC01 [∆phoP, ∆fad D26]University of Zaragoza, Institute Pasteur, TuBerculosis Vaccine Initiative (TBVI) HBHAInstitute Pasteur of Lille, INSERM, TBVI Hybrid 56Statens Serum Institute (SSI), Aeras, Intercell, TBVI HG85 A/BShanghai H&G Biotech Hybrid-I+IC31SSI, TBVI, Intercell M72GSK, Aeras MVA85A/AERAS-485Oxford-Emergent Tuberculosis Consortium (OETC), Aeras AERAS-402/ Crucell Ad35Crucell, Aeras M vaccae*Immodulon, NIH VPM 1002Max Planck, Vakzine Projekt Mgmt, TBVI rBCG30*UCLA, NIH, NIAID, Aeras AdAg85AMcMaster University Hybrid-I+CAF01SSI Hyvac 4/ AERAS-404SSI, Sanofi-Pasteur, Aeras, Intercell RUTIArchivel Farma M smegmatis* Prime Boost Post-infection Immunotherapy Preclinical vaccine candidates are not yet in clinical trials, but have been manufactured under Good Manufacturing Practice (GMP) for clinical use and have undergone some preclinical testing that meets regulatory standards. *indicates candidates that have been in clinical trials in the past, but are not currently being tested in clinical trials Source: Tuberculosis Vaccine Candidates – 2009; Stop TB Partnership Working Group on New TB Vaccines
Progress in TB Vaccine Development • 12 candidates have entered clinical trials; 9 currently being tested; 10th will enter trials this year • Robust pipeline of candidates in preclinical development • Capacity and infrastructure developed or being developed at several sites, including South Africa, Kenya, Uganda, Mozambique, Ethiopia, Senegal and the Gambia • Manufacturing capacity being developed and agreements explored, with particular emphasis on emerging economies • Regulatory pathways and market/economic impact research laying groundwork to accelerate adoption and uptake of new TB vaccines
Approach to a New TB Vaccine • Improve BCG – make a recombinant rBCG • Prime-Boost regimen • Give booster vaccinations in infants • Give booster vaccinations in adolescents who have received BCG at birth
Aeras TB Vaccine Candidates in Clinical Trials Potential Boost Vaccines • All vaccine candidates found to have acceptable safety profiles • All candidates induced CD4+ and/or CD8+ T-cell responses to TB antigens • Immunogenicity results of booster candidates after BCG-priming are encouraging for post-BCG prime-boost strategy
Clinical Trials: Field Site Development • Large-scale community-based clinical trials are conducted in high burden countries • Aeras partners with local research institutions to establish field sites and conduct clinical research • Build local infrastructure and health care/research capacity to perform future Good Clinical Practice (GCP) compliant Phase III clinical trials
Aeras Partnerships for Field Research St John’s Research Institute, India Cambodian Health Committee, Cambodia Makerere University, Uganda KEMRI/CDC, Kenya Manhica Health Research Centre Mozambique SATVI/UCT, Aurum Institute, UCT Lung Institute, South Africa
Site DevelopmentSouth Africa • Partnership with South African Tuberculosis Vaccine Initiative (SATVI) • Field site developed in Worcester (~120 km from Cape Town); most advanced site in the world for TB vaccine trials • Infrastructure developed: • State-of-the-art immunology laboratory • Highly skilled staff capable of performing the duties necessary to maintain the infrastructure and execute clinical research • Clinical and office facilities • Professional Development Program (Siyantinga- “Reach for the Stars”) – over 230 staff trained since 2004 • Resource Center
Aeras-Sponsored Trials in South Africa • SATVI is conducting Phase I, II and IIb studies of four vaccine candidates in Worcester • UCT Lung Institute conducted a Phase II clinical trial in adults with active or previous TB in Cape Town • Aurum Institute isenrolling adults living with HIV in Phase IIb trial in Klerksdorp (mining community)
Key Accomplishments at Other Partner Sites State-of-the-art immunology and mycobacteriology laboratory established in India Mycobacterial lab capacity is being augmented in Kenya and Uganda Local staff trained in clinical research in Kenya, Uganda and India Epidemiological cohort studies in Cambodia,India,Kenya and Uganda Quality management and data management infrastructure developed in India and Uganda New state-of-the-art Clinical Research Center established at a District Hospital in western Kenya First multicenter TB vaccine clinical trial initiated in Kenya
Local Benefits of Clinical Research • Retain local talent and expertise • Raise awareness about TB in the community • Support and enhance local clinical research capacity • Community health and education • Infrastructure remains in the community • Leverage investment in infrastructure to use for clinical trials of other diseases
Access and Availability • Future access considered at every stage of vaccine development • Manufacturing • Guarantee by partners for sufficient production and affordable prices, or technology transfer • Manufactured by Aeras with partners in developing world • Aeras will not consider vaccine candidates that will be costly to manufacture on a large scale • Pricing • Dual pricing for affordable distribution in resource-poor countries • Cost plus purchase from partner • Aeras provides at cost • Distribution • Developing country governments • International organizations (GAVI, UNICEF) • Developing country partners
Demand from Endemic Countries • Market study to analyze acceptability of 3 new pre-exposure vaccine scenarios • 86 respondents – govt., providers, NGOs • Interviews conducted in 8 high TB burden countries: Brazil, Cambodia, China, India, Mozambique, Romania, Russia, South Africa
Drivers of Future Uptake • Wide recognition that TB is serious and neglected problem; MDR-TB threat • Widespread dissatisfaction with current BCG • Likely demand for partially effective vaccine better than BCG • Willingness to commit to rapid introduction • FDA or EMEA approval will speed adoption • Willingness to spend money out of existing budgets for prime-boost; private sector
Barriers to Future Uptake • Clarify expected benefits (20-30 years) • Fatalism about TB– lack of political will and competing priorities, e.g., HIV/AIDS • Waiting for strong efficacydata, especially in own country • Some resistance to adolescent boosting (transient populations) • Some skepticism about aerosol delivery
Lessons Learned • Heterogeneity of responses within and between countries • Strong efficacy datawill be a critical success factor for introduction, including in-country data • Cost, if kept low, not likely to be major issue; not an issue in private markets • Education and preparation will be necessary, but raising awareness and expectations too high needs to be avoided
Join Us for a TB Vaccine Press Briefing“Eliminating TB: the promise of new TB vaccines” • WHAT: An update on the state of TB vaccine development, outcomes from the recent global science meeting on TB vaccines, and plans for the future. • WHO: • Kenyan TB Advocate Lucy Ghati • Dr. Joris Vandeputte, TBVI • Dr. Lew Barker, Aeras • WHERE: Press Briefing Room 42 • WHEN: 10 am - Monday, 15 November
Aeras gratefully acknowledges the support of the following major donors Netherlands Ministry of Foreign Affairs US Food and Drug Administration
Thank You! For more information: www.aeras.org pwillingham@aeras.org