Download
1 / 44
440 likes | 508 Views
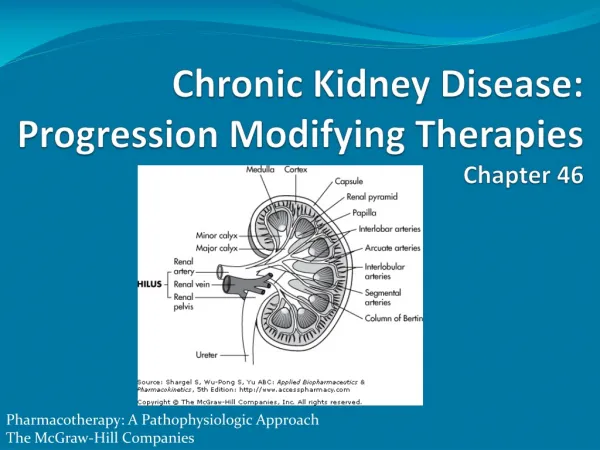
Kidney Disease Workup – When to refer to Nephrologist. Family Practice Review Feb 2013 4:30-5:30. Jeff Kaufhold MD, FACP Master Physician, Ohio University Heritage School of Medicine Nephrology Associates of Dayton. Renal Review.

E N D
Kidney Disease Workup – When to refer to Nephrologist Family Practice Review Feb 2013 4:30-5:30 Jeff Kaufhold MD, FACP Master Physician, Ohio University Heritage School of Medicine Nephrology Associates of Dayton
Renal Review • Now Kidney Disease- Work-up & When to Refer to a Nephrologist - What Drugs Not to Prescribe and What Drugs Work for HypertensionMark D. Oxman, D.O. • 5:30 p.m. - 6:30 p.m.Cloudy with Occasional Chance of Crystals: What You CanLearn from the Urine (Clinical Significance & Billing Codes and Reimbursment)Mark D. Oxman, D.O.
Pre Test • Which Treatment has the LEAST impact on progression of renal disease? • A. Use of ACE inhibitors • B. Referral to a nephrologist • C. Use of DHP calcium Channel Blocker • D. Control of Diabetes to A1c < 8.0 • E. The nature of the underlying renal Disease
New TerminologyARF - RIFLE criteria • Risk low uop for 6 hours, creat up 1.5 to 2 times baseline • Injury creat up 2 to 3 times baseline, low uop for 12 hours • Failure Creat up > 3 times baseline or over 4, anuria • Loss of Function Dialysis requiring for > 4 weeks • ESRD Dialysis requiring for > 3 months
CKD prevalence in world Populations • Country Population CKD est. • China 1.298.847.624 35.336.295 • India 1.065.070.607 28.976.185 • Indonesia 238.452.952 6.487.322 • Pakistan 159.196.336 4.331.076 • Philipines 86.241.697 2.346.281 • Vietnam 82.662.800 2.248.914 • Assumes 2.72 % incidence
CKD Stages • Stage 1. Normal function with known dz • Stage 2. GFR 60-80 • Stage 3. GFR 30-60 • Stage 4. GFR 15-30. • Stage 5. GFR less than 15. • Stage 6. ESRD on dialysis.
US Population with CKD Coresh, Selvin, Stevens. Prevalence of CKD in the US. JAMA.2007;298(17)2038.
Approach as CKD progresses GFR ----Stage 3--- Stage 4 Stage 5
Manage CRF Stages 1, 2, 3. Control BP Preferentially with ACE Control Diabetes with Target A1c < 8, based on the DCCT, ideally < 6.5 Careful with drug dosing Prevent Hyper PTH Vit D Calcium acetate Phosphate binder Diet Education Preparation of the Patient
Manage Fluids Dialysis education Access Placement Prevent anemia Prevent Malnutrition Start ACE? metolazone NKF program AV fistula, PD cath Epogen, Iron This can get tricky Stop ACE? Preparation of the PatientStage 4 and 5
Medical treatment in CKD Which drugs To avoid, and Which drugs Work for HTN
What Drugs to Avoid • Drugs to avoid when GFR is less than 40: • NSAID’s • Bactrim • IV Contrast • Fleets Enemas • Metformin, Xarelto • For GFR less than 30, need to be careful with combinations of drugs like ACE and Spironolactone.
Which Drugs work for HTN? • Global treatment of HTN • Use of Common Medications in CKD • Steps to improve survival in CKD • Nephrologists approach to Hypertension Treatment.
Nat’l Health & Nutrition Exam Survey NHANESControl of Hypertension JNC 7 Dec 2003
Medicare Part D & MarketScan CKD patients with at least one claim for an ACEI/ARB/renin inhibitor in the 12 months following the disease-defining entry period, by CKD diagnosis code, 2008Figure 2.14 (Volume 1) Point prevalent Medicare CKD patients age 65 & older & MarketScan CKD patients age 50–64.
Medicare Part D & MarketScan CKD patients with at least one claim for a beta blocker in the 12 months following the disease-defining entry period, by CKD diagnosis code, 2008Figure 2.15 (Volume 1) Point prevalent Medicare CKD patients age 65 & older & MarketScan CKD patients age 50–64.
Medicare Part D & MarketScan CKD patients with at least one claim for a DHP calcium channel blocker in the 12 months following the disease-defining entry period, by CKD diagnosis code, 2009Figure 2.16 (Volume 1) Point prevalent Medicare CKD patients age 65 & older & MarketScan CKD patients age 50–64.
Prevalence of comorbidity in NHANES 2001–2008 participants, by risk factor, expanded eGFR categories, & method used to estimate GFRFigure 1.5 (Volume 1) NHANES 2001–2008 participants age 20 & older. Note how HTN is bigger problem as GFR falls
Medicare Part D & MarketScan CKD patients with at least one claim for a lipid lowering agent in the 12 months following the disease-defining entry period, by CKD diagnosis code, 2008Figure 2.17 (Volume 1) Point prevalent Medicare CKD patients age 65 & older & MarketScan CKD patients age 50–64.
Mortality rates in NHANES 1999-2004 participants, by eGFR: MDRD equationFigure 1.11 (Volume 1) NHANES 1999–2004 participants age 20 & older.
Cumulative probability of a physician visit in the year following CKD diagnosis by physician specialty & dataset Figure 2.10 (Volume 1) Only about 30 % Patients alive and eligible all of 2008, CKD diagnosis represents date of first CKD claim during 2008, physician claims searched during 12months following that date.
How to improve CV Morbidity in CKD? 1. Early referral to Nephrology 2. Consider a patient with CKD 4 , 5, and ESRD as having the same risk as a patient who HAS ALREADY HAD THEIR FIRST HEART ATTACK. Beta Blocker Aspirin Statin restart ACE inhibitor or ARB once pt on dialysis To prevent a vessel wall thrombus
Hypertension Case Presentation • 56 y.o. A.A. male prior weight lifter presents for refractory HTN. • Normal labs and UA. Normal CXR and EKG. • Meds: Clonidine 0.2 BID • ACE inhibitor • Diltiazem 300 mg daily
Case Presentation • Physical Exam: • BP 170 / 110 Pulse 85 • Edema 2 +
Case Presentation • Special populations help define your approach. • African Americans: • CHF • Diabetics:
Case Presentation • Special populations help define your approach. • African Americans: Volume Mediated, Low renin low Aldo. May respond better to diuretics. • CHF: ACE, Diuretics, B-blocker, ASA • Diabetics: ACE or ARB.
Case Presentation • 56 y.o. A.A. male with edema, HTN • Normal labs and UA. Normal CXR and EKG. • Meds: Clonidine 0.2 BID • ACE inhibitor • Diltiazem 300 mg daily • Whats Missing???
Case Presentation • 56 y.o. A.A. male with refractory HTN. • Meds: Clonidine 0.2 BID • ACE inhibitor - Stopped • Diltiazem 300 mg daily • I added HCTZ 50 mg daily.
Case Presentation • 56 y.o. A.A. male with refractory HTN. • Meds: Clonidine 0.2 BID • Diltiazem 300 mg daily • HCTZ 50 mg daily. • Still swelling, BP a little better. 156 / 100.
Case • 56 y.o. AA male with refractory HTN. • I changed diuretics to Lasix and ultimately added Zaroxolyn. • I get a call 3 days later: Swellings gone, but I can’t get out of bed – too dizzy! • He had lost 15 lbs.
Case Presentation • 56 y.o. A.A. male with refractory HTN. • Meds: Lasix 40 mg BID • Zaroxolyn 5 mg weekly • No swelling, BP 126 / 80. • Pt reports joint pain and swelling. What test do you order next?
Case • Uric acid level is 12 • Creatinine 1.4 • K 3.8 • Glucose 244 (nonfasting)
Case • Started Allopurinol for gout. • Pt started exercising and watching diet. • Sugars normalized without treatment.
Joint National Commission • JNC 1 1980 founded on HDFP • JNC 2 1984 Intro of ACE, alpha B. • JNC 3 1986 Special situations • JNC 4 1988 Many agents 1st line • JNC 5 1993 Back to stepped care. • JNC 6 1997 ACE for Diabetics • JNC 7 2003
HYPERTENSIONJNC VII Outline • Epidemiology of HTN • Evaluation of HTN • NON Pharmacologic treatments: Wt loss, diet, exercise, alcohol • Drug treatment • Special Issues in HTN
HYPERTENSIONJNC V • "Because diuretics and B-Blockers are the only classes of drugs that have been used in long-term controlled trials and shown to reduce morbidity and mortality, they are recommended as first- choice agents unless they are contraindicated or unacceptable, or unless there are special indications for other agents."
Normal Prehypertension Stage 1 Stage 2 < 120 / 80 120 -139 / 80-89 140-159 / 90-99 > 160 / >100 Stages of Hypertension
Treatment of Hypertension • Stage 1 or Single agent – HCTZ for most pts. B-Blocker for females/ high heart rate. • Stage 2 I start with DHP CCB (Nifedipine XL) • plus one or both of above. • Resistant HTN I look for CLASSES of agents
Classes of Antihypertensives • Diuretics • Rate control agents BBlocker, Verapamil, Diltiazem • ACE/ ARB’s • Vasodilators Dihydropyridines, Hydralazine, Alpha blockers, Minoxidil • Central agents: clonidine, aldomet.
Nephrology level htn • I tell the pt that we’ll need to control the main route plus the main detours causing the HTN. • Average of 3.1 medications to achieve control • Rate control (pulse < 78) • Diuretic • Vasodilator DHP CCB, Hydralazine, Cardura, Minoxidil. • ACE / ARB (accept 30% increase in creat if BP responds)
Refer to Nephrologist • If unable to control on 3 drug regimen which includes Rate control, diuretic. • If you are considering Minoxidil or renal angio. • If creatinine climbs more than 30 % or if creatinine is over 2.0.
Post Test • Which Treatment has the LEAST impact on progression of renal disease? • A. Use of ACE inhibitors • B. Referral to a nephrologist • C. Use of DHP calcium Channel Blocker • D. Control of Diabetes to A1c < 8.0 • E. The nature of the underlying renal Disease