Download
1 / 22
220 likes | 645 Views
Medicare Part D Prescription Drug Benefit Presentation to: Health & Human Resources Subcommittee House Appropriations Committee Patrick W. Finnerty Department of Medical Assistance Services September 18, 2005 Richmond, Virginia Presentation Outline

E N D
Medicare Part D Prescription Drug Benefit Presentation to: Health & Human Resources Subcommittee House Appropriations Committee Patrick W. Finnerty Department of Medical Assistance Services September 18, 2005 Richmond, Virginia
Presentation Outline Overview of Medicare Part D & “Extra Help” for Low-Income Persons Impact on Virginia Implementation Activities
Medicare is a Federal Health Insurance Program • Eligibility for Medicare • 65 years or older and eligible to receive Social Security; • Under 65 years, permanently disabled, and have received Social Security disability payments for at least two years; • Have permanent kidney failure or need a kidney transplant; or Amyotrophic Lateral Sclerosis (or Lou Gehrig’s disease) • What Medicare Covers • Part A: Hospital Inpatient Care (also some skilled nursing facility care, home health, and hospice) • Part B: Medical Insurance (such as doctors’ services, labs, medical equipment, preventive services) • Part D: Prescription Drugs beginning on January 1, 2006
What Is Medicare Part D? • Medicare Modernization Act (MMA) enacted in December 2003 adds a new Part D to provide prescription drug coverage • Prescription drug benefit available to all Medicare beneficiaries on January 1, 2006 • Enrollment is optional, though a penalty may apply for late enrollment (enrollees must apply for coverage) • Prescription drugs available through private prescription drug plans (PDPs) • Most enrollees will have cost sharing obligations; “extra help” (subsidy) is available for low-income individuals
Who In Virginia Is Affected By Medicare Part D? • There are roughly 947,000 Medicare beneficiaries in Virginia • Approximately 136,000 Medicare beneficiaries are also Medicaid clients, called “dual eligibles” • 93% of Medicaid elderly clients are “duals” • 62% of Medicaid blind & disabled clients are “duals” • When Medicare Part D becomes effective, “dual eligibles” will receive their prescription drug coverage through Medicare, and not Medicaid
What is the MedicarePart D Benefit? • Prescription drug plans (PDPs) must offer a basic prescription drug benefit • Medicare Advantage plans (managed care plans) must offer basic plan or broader coverage at no extra cost • PDPs must provide coverage for drugs in each therapeutic class, but can establish preferred drug lists • Will include: drugs dispensed by prescription, insulin & associated supplies, vaccines • Will exclude: drugs covered under Part A or B, over-the-counter drugs, weight gain/loss; cosmetic purposes; cough & cold; barbiturates; benzodiazepines; certain vitamins (Va. Medicaid will continue to cover excluded drugs for “duals” for which we receive FFP)
How Are Prescription Drug Plans Selected/Monitored? • The Centers for Medicare and Medicaid Services (CMS) will contract with private health plans and other vendors to provide the Medicare Part D benefit • Virginia will have at least 2 PDPs; Medicare Advantage (MA) Plans (managed care) will also be available • CMS will require PDPs and MA Plans to meet certain quality, access and administrative standards (e.g., at least 2 drugs must be available in each drug class; 60-day notice for drug changes; network pharmacy access standards; P&T Committee requirements; and appeals process)
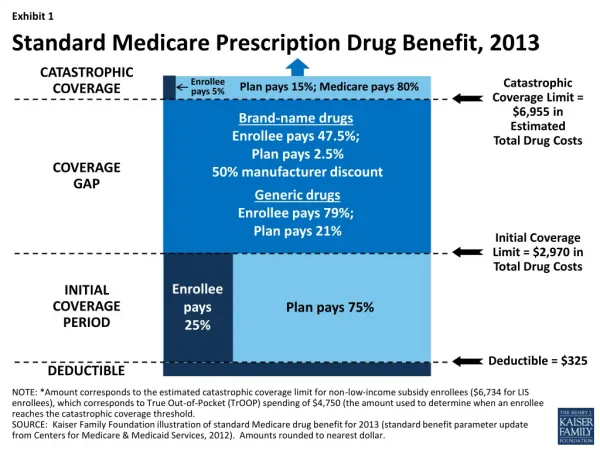
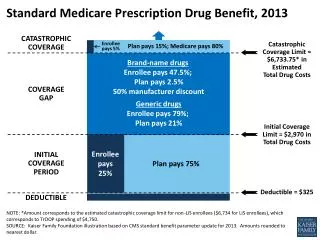
What Are The Cost-Sharing Requirements? • Under the standard prescription drug benefit, most beneficiaries in 2006: • Pay an average monthly premium of $34 • Pay the first $250 in drug costs (deductible) • Pay 25% of total drug costs between $250 and $2,250 • Pay 100% of the costs between $2,250 and $5,100 in total drug costs (this $2,850 gap is known as the “doughnut hole”), equivalent to $3,600 out of pocket. • Pay the greater of $2 for generics, $5 for brand drugs, or 5% coinsurance after reaching the $3,600 out-of-pocket limit • These deductibles, benefit limits, and catastrophic thresholds are indexed to rise with the growth in per capita Part D spending.
Certain Beneficiaries Will Receive “Extra Help” To Offset Cost of Prescription Drug Benefit • Group 1: Full benefit “Dual Eligibles” with income <100% Federal Poverty Level (FPL) ($9,570/year); no resource limits • Group 2: Persons with income <135% FPL ($12,920/year), and limited resources ($6,000/individual; $9,000/couple) • Group 3: Persons with income <150% FPL ($14,355/year), and limited resources ($10,000/individual; $20,000/couple)
How Do Persons Enroll in Medicare Part D Drug Coverage? • Medicare beneficiaries will need to enroll with a PDP or MA plan • Enrollment begins November 15, 2005 • Full-benefit dual eligibles who do not enroll in a plan by 12/31/05 will be auto-enrolled in a PDP • Can change PDP at any time • Information/assistance is available for beneficiaries: • Consult Medicare & You 2006 Handbook • Contact PDPs for information • Call Medicare toll-free 1-800-MEDICARE • Visit www.medicare.gov
How Can Persons Find Out If They Qualify For “Extra Help?” • Medicare beneficiaries apply to the Social Security Administration (SSA); persons can apply multiple ways • Scannable application (mail or in-person) • Calling SSA toll-free (1-800-772-1213) • Over the internet (www.ssa.gov) • “Qualifier Tool” • SSA is sending applications to those it believes may be eligible; others must initiate application process • States must determine eligibility for “Extra Help” if the applicant insists • Virginia will use same SSA application
Certain Low-Income Persons Are Deemed Eligible for “Extra Help” • Certain Medicare beneficiaries will automatically qualify for and receive “extra help” • No application is required for: • “Dual eligibles” • Supplemental Security Income (SSI) recipients • Those deemed eligible for “extra help” are identified through data sharing between DMAS and CMS
Important Dates forMedicare Part D Implementation • January 28, 2005 Final federal regulations published • February 2005 CMS Public Awareness Campaign begins • May 2005CMS Notifies Potential Low Income Eligibles • June 2005 Prescription Drug Plans Bids Due States submit enrollment files • July 2005 States/SSA accept low income applications • Sept. 15, 2005 Prescription Drug Plan Contracts Awarded • October 1, 2005 Marketing/enrollment of Part D benefits • November 15, 2005 Enrollment Begins; lasts until May 15, 2006 • January 1, 2006 Part D Begins; Medicaid payment ends 12/31 • February 2006 States’ monthly payment (clawback) begins
Presentation Outline Overview of Medicare Part D & “Extra Help” for Low-Income Persons Impact on Virginia Implementation Activities
Administrative/Operational Implications • Local Departments of Social Services (LDSSs) have significant new responsibilities related to “Extra Help” program • (will be addressed in Commissioner Conyers’ presentation) • There are also implications for DMAS: • Assist transition of “dual eligibles” to Part D • Provide monthly data to federal government • Handle increased telephone inquiries from “duals” • Provide “coordination of benefits” information • Conduct additional appeal hearings related to “extra help” determinations • Final cost impact still being determined
States Must Pay A Significant Portion of The Part D Drug Benefit • Phased-Down State Contribution “Clawback” • States are required to help finance Medicare Part D by paying the federal government the state share of the cost of prescription drug coverage for “dual eligibles” • State share is set at 90% of costs for 2006 and decreases to 75% by 2015 • “Clawback” amount based on: • Per capita costs for “dual eligibles” in 2003 • Per capita growth in drug spending nationwide since 2003 • Number of “dual eligibles” enrolled in Part D
Virginia’s “Clawback” Amount Does Not Recognize Recent Pharmacy Program Savings • Since 2003, Virginia has implemented several pharmacy savings initiatives that are not reflected in the “clawback” amount • Preferred drug list • Mandatory generic substitution • Threshold program • Maximum allowable cost (MAC) pricing for generics • Expanded drug utilization review (DUR) program • While the net impact of the “Clawback” amount is not supposed to impose additional costs to states, because post-2003 cost savings are not recognized, it appears that paying the “clawback” will be more expensive than continuing the current program
As A Result of Several Factors, It Appears Medicare Part D Will Incur Additional Costs for Virginia • Initial estimates indicate the overall impact of Part D for Virginia could reach $22 million (GF) in calendar year 2006 ($11 million for FY 2006) • Largest factor contributing to the cost is the “clawback” payment • Other factors include administrative costs and “woodwork” effect • DMAS is working with CMS to reduce impact of “clawback” payments • Final cost estimates are still being determined and will be considered carefully in developing the Executive Budget
Presentation Outline Overview of Medicare Part D & “Extra Help” for Low-Income Persons Impact on Virginia Implementation Activities
HHR Agencies Are Working Together Closely To Assist CMS/SSA Implement Part D • DMAS has formed a Medicare Part D Task Force • Over 75 individuals are participating, including federal and state agencies, LDSSs, provider associations, advocacy groups, and others • HHR agencies are completing necessary computer system changes • Information provided to General Assembly members • Communicating with “dual eligibles” • Providing training programs/materials
Training & Other Activities • An all-day training program featuring CMS and SSA staff was provided via videoconference to 29 sites across the Commonwealth yesterday • Training on Part D and “Extra Help” • More than 500 attendees • Videoconference was recorded on DVD; copies were made available for interested parties and information has been posted on agency internet sites • HHR agencies will continue to help the federal government implement the Part D program