Download
1 / 31
310 likes | 435 Views
Preventing delayed transfers of care: person-centred voluntary sector services. Dr Fiona Zinovieff, Dr Catherine A Robinson, and Dr Bryan Collis. f.zinovieff@bangor.ac.uk c.a.robinson@bangor.ac.uk bcollis@wcva.org.uk. Planning for the future.

E N D
Preventing delayed transfers of care: person-centred voluntary sector services Dr Fiona Zinovieff, Dr Catherine A Robinson, and Dr Bryan Collis f.zinovieff@bangor.ac.uk c.a.robinson@bangor.ac.uk bcollis@wcva.org.uk
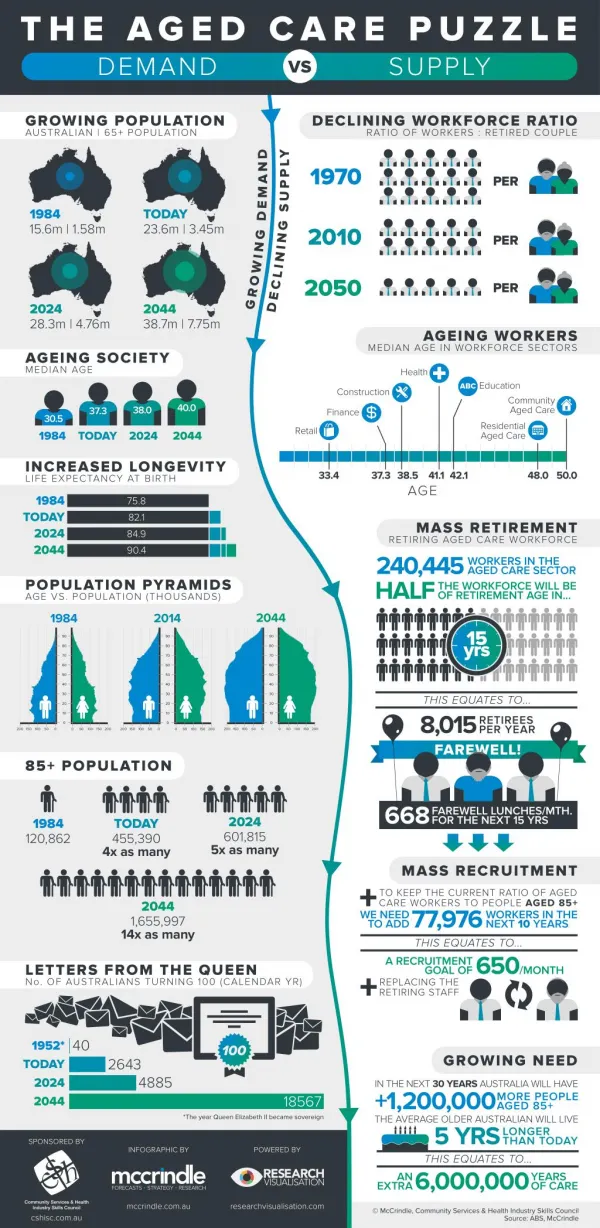
Planning for the future • Demographics predict per capita budget drops in statutory sector funding over next 10-15 years • Service commissioning drive • Economy • Efficiency • Effectiveness
Where to make savings? • Cut costs per capita • treat more people for the same money (or less money) • Provide additional services for the same price • added value increasing efficiency and effectiveness • Make people pay for at least some of their care
Voluntary Sector and added value Voluntary Sector ethos is holistic service But • Do the economics add up? • Is there evidence that voluntary sector services bring added value? • What is the added value? Welsh Assembly Government funded this research to provide an evidence base
British Red Cross: Home from Hospital, Out-of-hours transport, Equipment Loan Based in 1 hospital, serves 2 counties, Volunteers co-ordinated by paid staff Funded by 2 Local Authorities, 2 LHBs, supplemented by BRC Twilight Service: Out-of-hours transport and assessments & referrals Serves 2 hospitals within one NHS Trust Paid staff Funded by Local Authority, LHB and NHS Trust Two case studies: Preventing Delayed Transfer of Care
Case study 2 • Annual running costs (2008-2009) = £90,242 • Average cost of a bed day = £363 • Annual costs = 248 bed days* (*20.6 bed days per month)
The bottom line: Case study 2 Figures over a six month period 123 beds ‘created’ (96 avoiding unnecessary admission 27 preventing DTOC from CDU/SDU) 216 people transported home from hospital 25 additional referrals to other services
Case study 2: all this plus Reducing human suffering • Avoids admission to hospital • Prevents DTOC • Transport and Escort • Befriending • Settling service • Risk Assessment in the home
Case study 1 Annual running costs (2008-2009) £26,515 Cost of a bed night = £387 (fully absorbed) Annual running costs = 69 bed nights
Case Study 1: the bottom line 344 referrals to home from hospital 136 wheelchair loans 239 signposted to other agencies
Measuring added value Triangulating perceptions of: • Service providers • Management, Staff, Volunteers • Referring agencies • NHS, Social Services • Service users
What is added value? • Filling a gap • Person centered provision • Promoting independence • Signposting other services • Emotional support • Befriending • Flexible service • Fast response time • Reliable service
Case study 1: Filling a gap • Where there are no services • Where there are delays in obtaining services • Where an individual does not meet criteria for statutory services • Bridging between different service providers, health and social services
Case study 1: Filling a gap in services ‘They (carers from social services) come early in the morning and wash you and get you dressed and make sure you have lunch. Then if you want them to make anything or do anything they will. They don’t do major shopping but they’ll go for milk or bread or little things’ (Service user) ‘Years ago home help or home care they could do the shopping’ (Social worker) ‘I do shopping for people, I’ll take …either take them or go for them’ (Volunteer)
Case study 1: Filling a gap in service provision ‘When we go and see people and we do our assessment and you then have to say “Well I’m sorry, you don’t come into the eligibility criteria, but we can offer you this: it’s a voluntary service for up to six weeks” People are more than grateful and it gives them a little something’ (Social worker) ‘Fair play, I couldn’t have managed without them that’s for sure’ (Service user) ‘That service was superb. It was a lifesaver, absolutely superb’ (Service User)
Case study 1: Filling a gap caused by delays ‘If people are being assessed by social services they still have to wait to be assessed and we do have social service time scales… which is to respond within 48 hours of someone being medically fit and then we’ve got up to 5 days if they need a care package, but of course if its … the Red Cross then we can respond on that date…(Social Worker) ‘If somebody is going home on a Friday, I can put “Urgent” on the actual form and I can phone … then they [BRC] will go straight out on that same day or night and they will go and collect some milk and things’ (NHS staff)
Case study 1: Filling a gap: Wheelchair loans in the community (1) • ‘When my husband was very ill… he couldn’t walk and I couldn’t lift him and I managed to borrow a wheelchair from the Red Cross and then I could manage then. They [social services] said they would get me one from social services. The week he died they brought me a wheelchair… I’d waited a couple of months at least, a few months’ (Service user) • ‘More often than not we can get one [wheelchair] out to them the same day’ (Support worker)
Case study 1: Filling a gap: wheelchair loans (2) ‘If we don’t get the chair they can’t go home’ (Occupational therapist) ‘So they do it more ways than just for the patient they do it for the whole discharge planning process’ (Occupational therapist) ‘We haven’t coded anyone who has been delayed because of waiting for that type of equipment which I know BRC would be able to supply’ (Bed manager)
Case study 1: Filling a gap – wheelchair loans 3 • ‘Maybe they’ve got broken legs, broken arms, but they don’t fall into the category where we’d be able to get a wheelchair quickly from the wheelchair service. They need one for a few months, but they won’t need it long enough for them to supply one… Its usually that they can’t go home’ (Occupational therapist) • ‘As an OT department we used to have a lot of chairs we used to loan out to people, but they’ve just, you know, disappeared over the years.’ (Occupational therapist)
Filling a gap between services ‘I guess it’s up to nursing staff in that time, to talk to people about how they’re going to manage at home, to actually ascertain whether they need a referral to a social worker or referral to the Red Cross and, of course, the referrals to the Red Cross don’t need to come through social work’(NHS Staff) ‘The ones we get referred from carer support, from the rapid response, or from the hospital, if they haven’t social services, […] although they’ve refused it in the beginning, when the realise that we’re not interfering or we’re coming to the end, then they’re quite happy to go back to the social services and they accept their help, you see.’ (Support worker)
Person centered service • The ethos of the service is person centered. • It responds to individual needs • Flexible service delivery • elements of the package • timing of the services • Reliable service • punctual • personal
Case Study 1: Befriending • ‘Home care sometimes, it is a very quick, sort of in-out. You like to think it’s a little more personal … but they don’t have the time to spend with people. So a befriending service is quite crucial really for people that go home. People that live alone with no family, they might not have any other links so that sort of service is really good’ (Social Worker) • ‘He has time for people and he’s got a nice way with him’ (Service User)
Case Study 1: Person Centered – Befriending (2) ‘They really did look after me and the girl who was looking after me, she’s still in touch’ (Service User) ‘So, yeah, you do keep in touch and you do, um, try and find out how they are.’ (Support worker) ‘You don’t, sort of, intrude into their lives, you know… put a little card through at Christmas, hoping she was better’ (Volunteers)
Case study 1: Person centeredpromoting independence ‘I’m only 54 so I’ve a young attitude to life … So its hard to accept it and I won’t accept it [stroke]. So I wouldn’t go out for a while. It was good what they did’ (service user) ‘Maybe they’ve fallen a lot and then they think “Oh I can’t go shopping any more” and then when they’ve got someone to take them they think “Oh yes, I’m much better” and “Oh yes I can do that” and it gives them more confidence” (NHS staff)
Case study 1: Person CenteredPromoting independence (2) ‘You’ve got to gauge, really, I feel, with some older people, um… you’ve got to be very careful. I had one lady, and she would struggle, she was definitely a candidate for the wheelchair …And this old lady was so proud and …That day there was one (wheelchair) for her but she would rather struggle. … But she made it back, you know? Very proud lady, well in her eighties. Hmm.’ (Support Worker) ‘We don’t like people to go shopping for us. We like to be able to choose our own thing’ (Service User)
Case study 1: Person Centered Reliable service ‘Yes I used them (BRC) to go to the hospital to keep appointments because the ordinary hospital transport was sometimes late coming. Or else it picked up people on the way, so you were always late.: That’s not too good, […] you could be very late and perhaps not have… It happened once there wasn’t any transport to bring me home… So I had to stop the night, yes.’ (Service User 8) • ‘It was reliable and pleasant’ (Service User 5) • That’s what I like, the reliability of it, you know. There’s no messing (Service User 10)
Case Study 1- Person centered service delivery ‘The ambulance brought me home … They dropped me at the gate… There is no heating… No, no one. … Hard, hardest thing I’ve ever, ever..thing I’ve had to do in my life because all your left side goes and I had limited movement in my left side …and I fall.’ (Service User) ‘He (BRC Volunteer) went in and saw there was a chair for me as well to go in, and you know he was ever so good. He really was. I was treated like a Queen! (Service User)
Case study 1: Person Centered Responding to individual need • ‘and she wanted to go into town and, you know, she didn’t actually say but you knew she was going for the last time. It was so sad. We went at lunchtime and luckily, we saw some of my ex-colleagues, and they cottoned on to what I was doing and jollied her along, which was lovely and she’d had a good day… well a couple of hours, you know. it was nice. That’s very worthwhile… I felt privileged, really, to have taken her shopping.’ (Volunteer)
Case Study 1: Ethic of service ‘You see you can have services provided by the state that could mean provided by aparatchiks, bureaucrats who are not really sympathetic, who are just doing a nine-to-five […] But as far as the voluntary sector is concerned I think they still have an ethic of service. There is something called the ethic of doing good. It makes a lot of difference, you see, and for them to do something which they consider to be good, whatever their motivation, […] I can see that. (Service User)
Conclusion Economic outcome: service for less than the cost of the bed days saved Efficiency outcome: helping ‘patient flow’-reducing waiting time breaches, reducing human suffering Effectiveness: preventing delayed transfers of care + Person centred ‘added value’
Thank you Fiona Zinovieff, CARES, Bangor University, f.zinovieff@bangor.ac.uk Catherine Robinson, CARES, Bangor University, c.a.robinson@bangor.ac.uk Bryan Collis, Wales Council for Voluntary Action, bcollis@wcva.org.uk