Download
1 / 41
420 likes | 700 Views
Interventions for Smoking During Pregnancy. Patricia Cluss, Ph.D. Pittsburgh Mind-Body Center Summer Institute 2007. Review of AHCPR/PHS Smoking Cessation Guideline (1996 & 2000). Effective smoking cessation treatments exist Every smoker should be offered an effective treatment

E N D
Interventions for Smoking During Pregnancy Patricia Cluss, Ph.D. Pittsburgh Mind-Body Center Summer Institute 2007
Review of AHCPR/PHSSmoking Cessation Guideline(1996 & 2000) • Effective smoking cessation treatments exist • Every smoker should be offered an effective treatment • Health care clinicians: screen for tobacco use status of every patient • Brief cessation treatments are effective; at least a minimal intervention should be provided to every smoker.
Effective Treatment • Three effective treatment elements: pharmacological aides, social support, skills training/problem solving • Dose-response relationship: More intense treatment = greater effectiveness • Identify and intervene with smokers at every health care visit
Pharmacotherapies • Nicotine replacement therapies (patch, gum, lozenge, nasal spray, inhaler) • Zyban (Wellbutrin/bupropion) • Chantix (varenicline)
Key components of programs for all smokers • Information • Behavioral problem solving skills • Coping strategies • Attention to motivation and readiness • Social support • Relapse prevention
The 5Asfor Health Care Settings • Ask • Advise • Assess • Assist • Arrange
5A Results • Provider Ask rates have increased from 10-30% a decade ago to about 60% in 2004. • Advice rates to identified smokers is about 70% now • Rates of the last 3 of the 5As continue to be poor.
Other Mnemonics / Plans • Ask, Advise and Refer • Ask and Act Expert committee has been reconvened for a guideline update within next several years
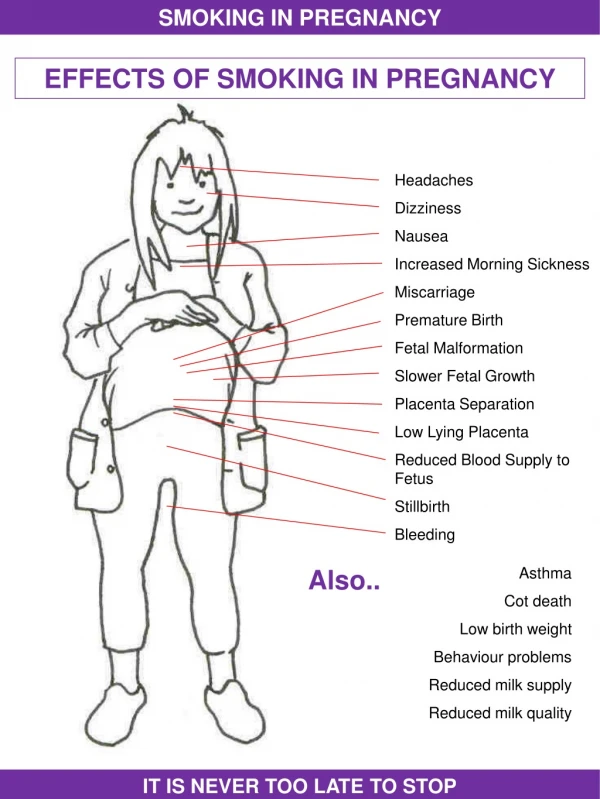
Health RisksSmoking during pregnancy is one of the major preventable risk factors for perinatal morbidity and mortality: • Intrauterine growth retardation (low birth weight, length, head circumference) • Increased risk for ectopic pregnancy, miscarriage and premature delivery • Adverse long-term effects on children’s neurocognitive development • Adverse effects on postnatal height growth • Postnatal impaired arousability from sleep (associated with SIDS)
Smoking during Pregnancy as a Health Care Crisis for the Underserved • Reducing smoking during pregnancy by 1% in U.S. over 7 years would prevent 57,000 LBW infants and save $572M in direct medical costs. • Low SES women are much more likely to smoke during pregnancy (23%) than higher SES women (5%). • At MWH prenatal clinic, 50% of pregnant women smoke.
How many women smoke during pregnancy? • Prevalence between 1987 and 1996 reduced from 16% to 12%. • Pregnant women are about half as likely as nonpregnant women to be smokers. • The median number of cigarettes smoked for pregnant women has remained a fairly constant 10/day.
Who smokes during pregnancy?(Race & ethnicity) % Source: National Center for Health Statistics
Who smokes most during pregnancy?Low SES women,regardless of how SES is measured • Least educated: high school or less • Lowest income: women on Medicaid are 2X as likely to smoke as those with private insurance • Of employed women, those with the lowest status jobs (5X greater than those with highest status jobs)
Who quits when pregnant? • 25% quit when they become pregnant (spontaneous quitters) • Lighter smokers • Older • Having their first baby • Smoking for a shorter amount of time • Higher education level • Higher SES • Partner who is a nonsmoker
The Good News With increased availability of information about the harmful effects of smoking, more women are aware of the value of quitting before or at the beginning of a pregnancy. The Bad News For those who don’t, it’s hard. The good news & the bad news
PHS Guideline recommendationsfor pregnant smokers: • Quitting any time during pregnancy is beneficial • More intensive interventions are preferred
Cutting Down as a Goal for Pregnant Smokers? Alcohol abuse Substance abuse Nonpregnant smokers Pregnant smokers: dose-response relationship
What works? • Tailoring the intervention for pregnancy • Brief counseling of 5-10 minutes • Nicotine replacement therapy, Zyban, or Chantix??????? • Provide cessation interventions for smoking partners??
Working with low SES pregnant smokers • Cessation programs are less effective for low vs. high SES smokers • Low SES women report more stressful events, more perceived stress, more negative appraisal from family, less social support & higher addiction to nicotine
These conditions result in lower: Motivation to stop smoking & Confidence in their ability to stop
Relapse • 15-30% relapse during pregnancy • 55-70% relapse within 1 year postpartum • 60% of those relapse within 1 month
Factors associated with relapse • Decreased motivation to be a nonsmoker in the postpartum • Decision not to breastfeed/short duration of breastfeeding • Concern about losing weight in the postpartum • Changes in social support for not smoking
Interventions for low SES pregnant smokers should include: • More intensive interventions • Focus on reducing stress • Identification of depression & other MH needs • Increased focus on social support • Attention to postpartum relapse
Problems with Screening During Pregnancy: • 14% of privately insured women do not disclose that they smoke • 25%-40% of women seen in public maternity clinics do not disclose
Improving the validity of self-report of smoking status “Do you smoke?” • I smoke about the same as or more than before I was pregnant • I’ve cut down since I found out I was pregnant • I have quit smoking since finding out I was pregnant • I wasn’t smoking around the time I found out I was pregnant and I don’t currently smoke
Pittsburgh’s Least Well-Known Claim to Fame: #1 in smoking during pregnancy of any large US City* Source: Annie E. Casey Fdn. Kids Count Special Report, 1999
The Pittsburgh STOP (Stop TObacco in Pregnancy) Program • An outcomes-driven evidence-based program for underserved pregnant smokers • Almost 900 pregnant smokers and recent quitters have participated since 2000 (60%/40%) • Based at WPIC with community outreach at Magee-Womens Hospital and other community locations
Pittsburgh STOP ProgramReadiness-based recruitment & intervention strategies Sure you can’t/don’t want to quit, but willing to think about cutting down? Thinking about quitting, but not sure? Ready to quit?
Pittsburgh STOP Program • Mean age 23; range from 14-42 • Marital status: 83% single • Education: 41% did not graduate HS • Income: 56% have yearly income < $10K • Insurance: 91% Medicaid or uninsured • # other children: avg. = 1; range 0-7 • Pregnancy unplanned for 85% • D&A: 35% admit concurrent use • Current domestic violence: 20%
STOP Program Innovative features in the STOP Program: • Incentives: • Small baby gift for attending sessions • Small gift for self for meeting cessation or cut-down goals • Exhaled air carbon monoxide (CO) monitoring
Originally built into the design as an evaluation measure to confirm self report of smoking status Initial concern about effect of this measure on participant-interventionist relationship CO Monitoring
Based on participant feedback, CO monitoring is now used as a program element to motivate change. CO Monitoring
STOP Participants’ CO LevelsAll those who entered as smokers A CO score of 8 or less is indicative of no smoking
Smokers’ Pre-delivery CO LevelsThose with 3 or more pre-delivery readings CO score of 8 or less is indicative of no smoking
CO Monitoring as a Motivator • Baseline score with printed and verbal info about how higher levels of CO/lower levels of oxygen affect the mother and the fetus • Used as an example of other harmful physiological effects of smoking on mother and fetus • Weekly CO goals • Chart for ongoing CO monitoring
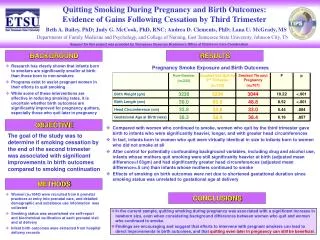
STOP Program Results • Drop out rate low at 14% • Quit & stay quit rates: • 26% quit rate for those who enter as current smokers; most who do not quit do cut down • 93% stay-quit rate for those who enter as recent quitters • Birth outcomes ex-smokers vs. smokers: • Significantly higher birth weights (11 oz.): only 13% born LBW vs. 24% for smokers (p=.02) • Longer gestational age (38 vs. 37 weeks): only 24% born preterm vs. 34% for smokers (p=.10)