Download
1 / 33
930 likes | 2.8k Views
The Edentulous Mandible: An Organized Approach to Implant-Supported Overdentures. Presented by:Dr.samaneh abbasi Supervised by: Dr. Mansour Rismanchian And Dr.saied Nosouhian Dental of implantology Dental implants research center Isfahan university of mediacal science.

E N D
The Edentulous Mandible: An OrganizedApproach to Implant-SupportedOverdentures Presented by:Dr.samanehabbasi Supervised by: Dr. MansourRismanchian And Dr.saiedNosouhian Dental of implantology Dental implants research center Isfahan university of mediacal science
The Edentulous Mandible: An OrganizedApproach to Implant-SupportedOverdentures
The continued bone loss after tooth loss and associated compromises in esthetics, function, and health, make all edentulous patients implant candidates. • The average denture patient does not see a dentist regularly. • The more often a patient wears a denture, the greater the bone loss • Yet 80% of denture patients wear their dentures day and night, which accelerates the bone loss.
The bone loss that occurs during the first year after tooth loss is 10 times greater than in following years. • In the case of multiple extractions, this often means a 4-mm vertical bone loss within the first 6 months. • Rather than waiting until the patient has lost most of the residual bone, the dentist should inform and emphasize to the patient the benefits of implants and why they should be inserted before the bone is lost.
The majority of mandibularoverdentures are supported by two implants anterior to the foraminae and soft tissue support in the posterior regions. Yet posterior bone loss occurs four times faster than anterior bone loss. • Reddy et al found prostheses completely supported by implants in the edentulous mandible actually may increase the posterior bone volume (even though posterior implants are not inserted)
The bone under an overdenture may resorb as little as 0.6 mm vertically over 5 years, and long-term resorption may remain at less than 0.05 mm per year • maxillary overdenture often provides improved support for the lips and soft tissues of the face • An implant-supported overdenturemay limit lateral movements and direct more longitudinal forces.(A mandibular denture may move 10 mm during function). • The complete denture group needed 1.5 to 3.6 times the number of chewing strokes compared with the overdenture group.:" The chewing efficiency with an implant overdenture .is improved by 20% compared with a traditional complete denture.
DISADVANTAGES OF IMPLANTOVERDENTURES • if a patient's primary request is not to remove the prosthesis, an implant-supported overdenturewould not satisfy the psychological need of this patient. • The mandibularoverdenture treatment plan requires more than 12 mm of space between crestal bone and the occlusalplane • greater long-term expenses than those with fixed restorations. Attachments such as O-rings or clips wear and must be replaced regularly • denture teeth wear faster on an implant overdenturethan with a traditional denture because bite force and masticatory dynamics are improved. • Continued posterior bone loss ,& may cause a combination-like syndrome, • food impaction. • Movement (RP-5)
Classification of Prosthesis Movement • no movement during function :PM-0 • hinge motion:PM-2 • apical and hinge motion:PM-3 • movement in four directions: PM-4 • all ranges of prosthesis movement:PM-6
If the prosthesis is rigid when in place but can be removed, the prosthesis movement is labeled PM-O, regardless of the attachments used.( O-rings are placed along a complete arch bar) • A hingelike prosthesis movement permits movement in two planes (PM-2)( the Dolderbar and clip without a spacer or Haderbar and clip) • If the Hader or Dolder bar is at an angle or parallel to the direction of desired rotation, the prosthesis is more rigid and may resemble a PM-O system
Dolder bar and spacer is desirable when greater amplitude of movement is needed to account for poorer ridge anatomy. An attachment system that permits apical movement and a hinge motion is called a type PM-3 system. • Magnets allowing a PM-4. An advantage is that they exert practically no lateral force on the implants. the implants usually must be independent from each other for this range of motion to occur • An O-ring or extracoronal resilient attachment may correspond to six directions of motion.
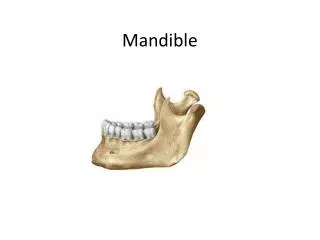
The greatest available height of bone is located in the anterior mandible, between the mental foraminae. This region also usually presents optimal density of bone for implant support. • overdentures with posterior movement (RP-5) gain better acceptance than removable restorations with anterior movement. • The available bone in the anterior mandible is divided into five equal columns of bone serving as potential implant sites, labeled A, B, C, D, and E, starting from the patient's right side
Overdenture Option 1 • patient's desires should also be minimal, and the bone volume should be abundant (Division A or B). • The posterior ridge form should be an inverted U shape, with high parallel walls • The problem associated with the existing denture relates primarily to the amount of retention. Under these conditions, two implants may be inserted in the B and D positions. • The implants remain independent • The most common type of attachment used in 0D-1 is an O-ring design,
independent implants in the A and E positions allow a greater amplitude of rocking of the restoration compared with implants in the B and D regions. When using B and D implants, the anterior movement of the prosthesis is reduced • the prosthesis may act as a splint for the two implants during anterior biting forces • only one implant is loaded at a time in most situations • The stability and support of the prosthesis are gained primarily from the anatomy of the mandible and prosthesis design
The patient's primary advantage with 0D1 is cost. • when arch shape is considerably tapered such that a connecting bar would be cantilevered too far to the facial or would interfere with speech and mastication if too lingual. • Hygiene procedures are facilitated with independent ball attachments
disadvantages of the 0D-1 • relatively poor implant support and stability • increase in prosthetic maintenance appointments. • If one implant is higher than the other, the prosthesis will disengage from the lower implant during function and rotate primarily on the higher implant • acceleration the wear of the O-ring or attachment on the lower implant. • increased risk of complications may occur, including abutment screw loosening, crestal bone loss, and implant failure • If one implant is more distal (farther from the midline), it will serve as the primary rotation point the more medial implant attachment will wear faster, and the more distal implant will receive a greater occlusal load.
Overdenture Option 2 • The implants are positioned in locations B and D and splinted together with a superstructure bar without any distal cantilever • Reduced loading forces are exerted on two anterior implants The two splinted implants should not be in the A and E.
If the surgeon inadvertently inserts the implants in the A and E position: • place at least one additional implant, usually in the C position • leave the implants independent with O-ring attachments. • Two implant overdentures are not indicated in C-h or D bone and are not indicated when opposing natural teeth.
Overdenture Option 3 • Three root form implants are placed in the A, C,E • A superstructure bar connects the implants, but with no distal cantilever
The implants splinted in the A, C, and E positions should not form a straight line. The C implant is anterior to the more distal A and E implants and directly under the cingulum position of the denture • If the posterior ridge form is poor (Division C-h), the lack of lateral stability places additional forces on the anterior implants. Implants then are best placed on the BCD position to allow greater freedom of movement of the prosthesis
Overdenture Option 4 • four implants are placed in the A, B, D, and E positions. • usually provide sufficient support to include a distal cantilever up to 10 mm on each side if the stress factors are low • Cantilevers may be compared with a class 1 lever. The distal most implant on each side acts as a fulcrum when occlusal forces are applied to the distal cantilever. • a 25-lb load to a lO-mm cantilever results in a 250-lb moment force. • if the two anterior implants are 10 mm from the fulcrum (distal implants), the effect of the posterior cantilever is countered.
implants are 5 mm apart, the mechanical advantage of the lever is the lO-mm cantilever divided by the 5-mm A-P spread, which equals 2. • A 25-lb distal force is magnified to 50lb to the anterior implant and 75lb • (50 + 25 = 75) to the distal (fulcrum) implant
Squarearch forms limit the A-P spread between implants and may not be able to counter the effect of a distal cantilever. • In a tapering arch A-P spread is often 10 mm and therefore often permits a cantilever up to 10 mm • In an ovoid arch, which is most common, the A-P spread between AE and BO is usually 8 mm. Therefore the cantilever may be up to 8 mm long distally from the A and E implants
The A-P spread is only one factor to determine the length of the cantilever. • When stress factors such as occluding forces are greater, the cantilever is decreased. • When the crown height is doubled, the moment forces are doubled. • Therefore under ideal, low-force conditions (crown height less than 15 mm, no parafunction, older females, opposing maxillary denture), the cantilever may be up to 1.5 times the A-P spread for 0D-4 overdentures.
five implants are inserted in the A, B, C, D, and E positions. • The superstructure is cantilevered distally a maximum of 2.5 times the A-P spread (if all the stress factors are low) and averages 15 mm, which places it under the first molar area
THE HIDDEN CANTILEVER • that portion of the cantilever that extends beyondthe connecting bar • If the prosthesis does not rotate at the end of the bar to load the soft tissue, a hidden cantilever exists • Therefore the cantilever length is measured to the point of prosthesis movement, not to the end of the bar and attachment system • When arch form or force factors do not permit an RP4 restoration with only implants between the foramenae, placing an implant in one of the first molar positions should be considered. This increases the A-P spread and results with only one cantilever.
DIVISION C-H ANTERIOR MANDIBLES • In the C-h anterior bone volume patient, one more implant is added to each option and OD-1 is eliminated completely. • Therefore OD-2 has three implants (A, C, and E positions), • OD-3 has four implants (A, B, D, and E regions), • 0D-4 has five implants (A, B, C, D, E areas), • OD-5 has six implants.
Overdenture bars may be cemented or retained with screws. • Three advantages of a cemented bar are the insurance of a passive superstructure, reduced cost, and an easier bar impression technique • stronger cements and a reduction of the cantilever length should be considered for 0D-4 and 0D-5 treatment plans because tensile forces may break the anterior cement seals and cause cornplications.